
Executive Summary
In the most recent state budget, Texas legislators allocated $200 million to Thriving Texas Families (TTF), a state program that aims primarily to “promote healthy pregnancy and childbirth” and “promote childbirth as an alternative to abortion,” among other goals.[1] However, the annual program report that outlines funding distribution and activities offers limited information connecting program activities to its aims. This analysis synthesizes publicly available materials to assess the alignment of the program’s work and its stated goals in the first year of the program.
Thriving Texas Families: An Overview
The TTF program broadly seeks to promote childbirth and provide support services to pregnant women, via performance outcomes including “improving healthy pregnancy and childbirth outcomes” and “improving child health and development.”[2] The program launched in 2023 as a codification and evolution of the decades-old state-funded Alternatives to Abortion (A2A) program, which began in the 2006–07 biennium with $5 million in Temporary Assistance for Needy Families funding.
The transition from A2A to TTF followed the passage and implementation of increasingly restrictive state-level abortion bans and substantial increases in general revenue (i.e., taxpayer dollars) budgeted for the program. When the Texas legislature relaunched A2A as TTF in 2023, it allocated $140 million for the 2024–25 biennium — more general revenue than the state’s Family Planning Program received in the same period — and increased the TTF budget to $200 million for the 2026–27 biennium.[3] TTF’s funding dramatically exceeds comparable state programs: in fiscal year 2026, the TTF budget will be more than three times larger than the $29.5 million allocated to the Florida Pregnancy Support Services Program, the next-largest comparable program.[4]
Figure 1 — Alternatives to Abortion (A2A) and Thriving Texas Families (TTF) Budget Timeline
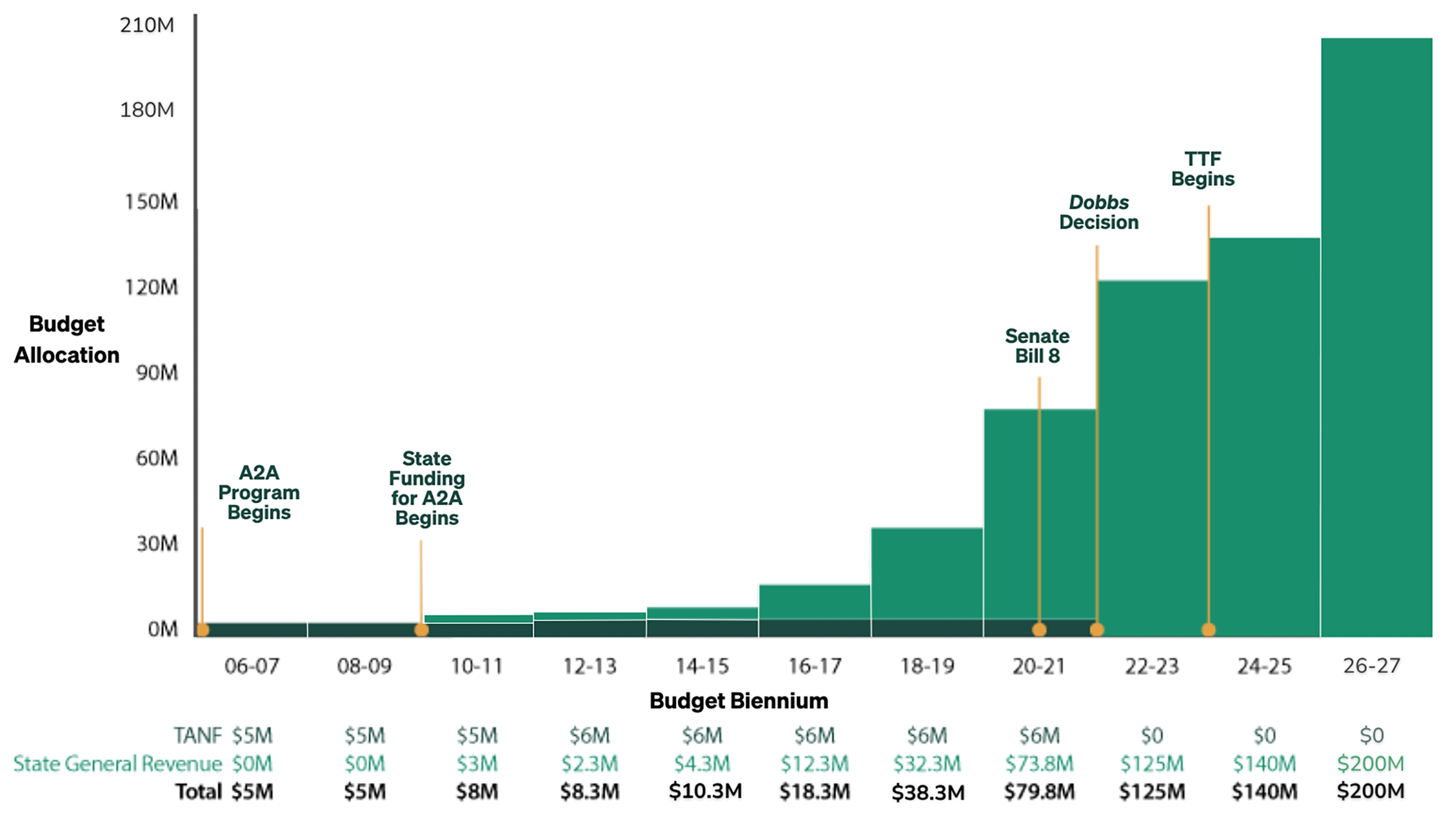
Note: SB 8 banned abortion early in pregnancy; the “Dobbs v. Jackson Women’s Health Organization” case led to the implementation of Texas’ abortion ban.[6]
Despite TTF’s stated focus on health, program guidelines exclude medical goods and services. Although non-medical services can improve the health of pregnant and postpartum women, this substantial state investment in exclusively non-medical services raises questions about alignment with a broader need for access to evidence-based reproductive health care in Texas. Reproductive-aged Texans have:
- Persistently low rates of preferred contraceptive method use, which makes it difficult for people to prevent unwanted pregnancies.
- Low rates of timely access to prenatal care.
- High rates of teen and repeat teen births.
- High rates of maternal mortality.[7]
Texas also has the highest rate of uninsured women in the country, and the rate may rise as the Affordable Care Act enhanced subsidies expire in 2026.[8]
Annual reports that outline program funding distribution and activities each year provide limited information connecting program activities to specific aims. An external program impact evaluation, required by SB 24, has been delayed by a lack of viable applicants and remains unreleased as of March 2026.[9] To address these gaps, this analysis synthesizes publicly available materials — including the fiscal year 2024 (FY24) report and the 2020 A2A Request for Applications (RFA) — to evaluate how the program’s distribution of funds and services aligns with its stated goals.
Objectives and Grantee Profiles
For FY24 (September 2023–August 2024), the funding period considered here, the RFA solicited applications toward the following specific goals: “reduce abortions and improve pregnancy outcomes by helping women practice sound health-related behaviors and improve prenatal nutrition; improve child health and development by helping parents provide responsible and competent care for their children; and improve families’ economic self-sufficiency by helping parents continue their education and find a job.”[10]
The Texas Health and Human Services Commission awarded funding to four main grantees, each of which in turn distributed funding to subgrantees or sites. A separate set of pilot projects also received funding.
Recipients in FY24 were prohibited from “performing or promoting Elective Abortions; or being an affiliate of any entity or individual that performs or Promotes Elective Abortions.”[11] As of 2025, state law also prohibits TTF funding from being awarded to governmental or quasi-governmental entities, hospitals, or any organization that primarily functions as a medical, behavioral health, or mental health provider, unless it received funds before September 2023.[12] This exception applies solely to Longview Wellness Center, a federally qualified health care center, which is the only medical provider whose receipt of TTF/A2A funds predates this cutoff.
Program guidelines exclude medical goods and services, including pregnancy tests and ultrasounds, from TTF reimbursement.[13] Services and goods eligible for TTF reimbursement include counseling, mentoring, educational information, classes, non-medical goods, care coordination, call-center activities, housing, and support provided via maternity homes.[14]
In FY24, the four TTF grantee organizations collectively received $69.4 million and supported 188 brick-and-mortar locations, 12 mobile units, and two virtual sites (Table 1).[15]
Table 1 — Contract Awards and Sites by Main Grantees
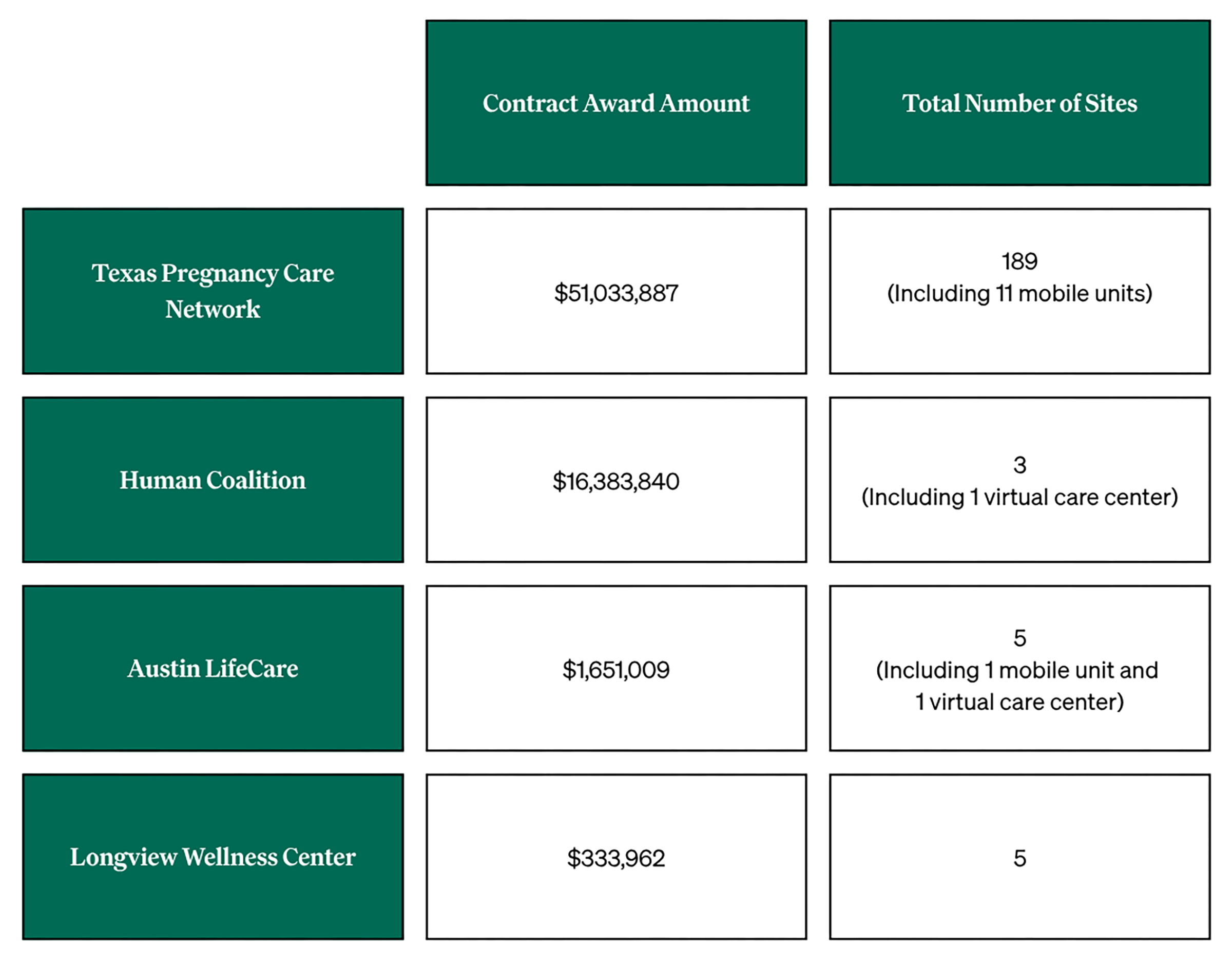
Note: Contract award amounts sourced from topline findings on the 2024 report. Pilot projects not included in contract award amounts or total number of sites.
Funding Distribution Favors Minimally Regulated Pregnancy Centers
According to their primary service model, analysis categorized the 202 non-pilot TTF-funded sites — including virtual and statewide locations — into the four types of sites named in the FY24 TTF report: pregnancy centers, social service providers, maternity homes, and adoption agencies. This classification was based on 2022 A2A site service classification data and a review of grantee websites.[16]
The 102 TTF-funded pregnancy centers constituted 51% of FY24 TTF sites and received 60% of TTF funds. Of these, 95% were identified as crisis pregnancy centers (CPCs), sites that seek to convince pregnant people to stay pregnant, often operating from an evangelical Christian mission.[17] Also referred to as “pregnancy resource centers,” “unregulated pregnancy centers,” and “anti-abortion clinics,” they advertise free services such as pregnancy tests (generally over-the-counter urine tests) and limited, non-diagnostic ultrasounds.[18]
These centers are unlikely to achieve TTF’s stated aims for a number of reasons:
- Research and other investigations have found that CPCs are rarely staffed by licensed medical professionals who regularly provide medical services at the center, and because few are medical facilities, typically client data is not protected by privacy laws such as the Health Insurance Portability and Accountability Act (HIPAA).[19]
- Studies show, moreover, that CPCs rarely provide effective education on important elements of reproductive health, and their use of deceptive and misleading tactics may generate confusion or delays in accessing prenatal care.[20] For example, many CPCs seek to intervene in pregnancy decision making by distributing medically inaccurate information about abortion and the efficacy of contraception.[21]
- Research also shows that CPCs rarely shape pregnancy outcomes.[22]
- Texans still access abortion by traveling out of state or obtaining medication abortion by mail. In 2024, more than 27,700 Texans traveled out of state for abortion care, and over 35,800 obtained abortion medications online.[23]
Table 2 — Distribution of TTF Funding
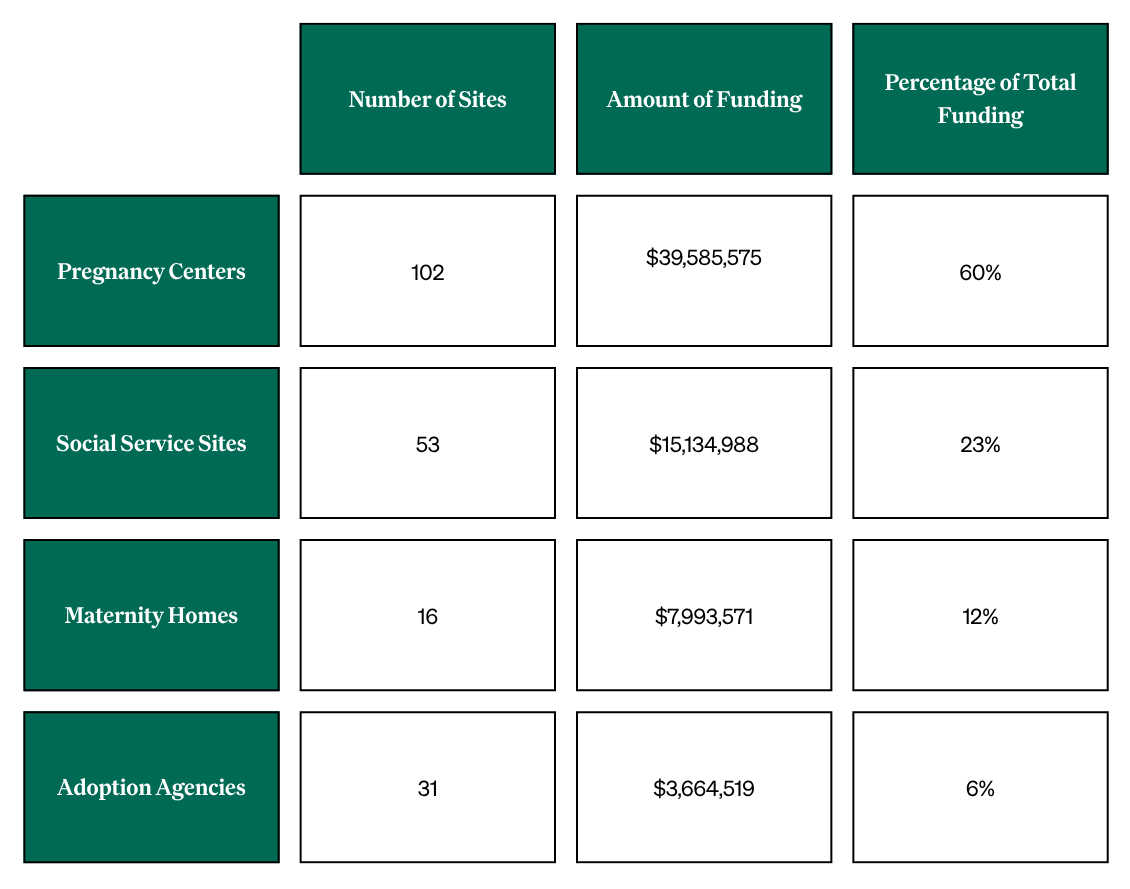
Note: The table is based on analysis of the 2024 report. Percentages may not total 100% due to rounding.
Service Alignment with Program Aims
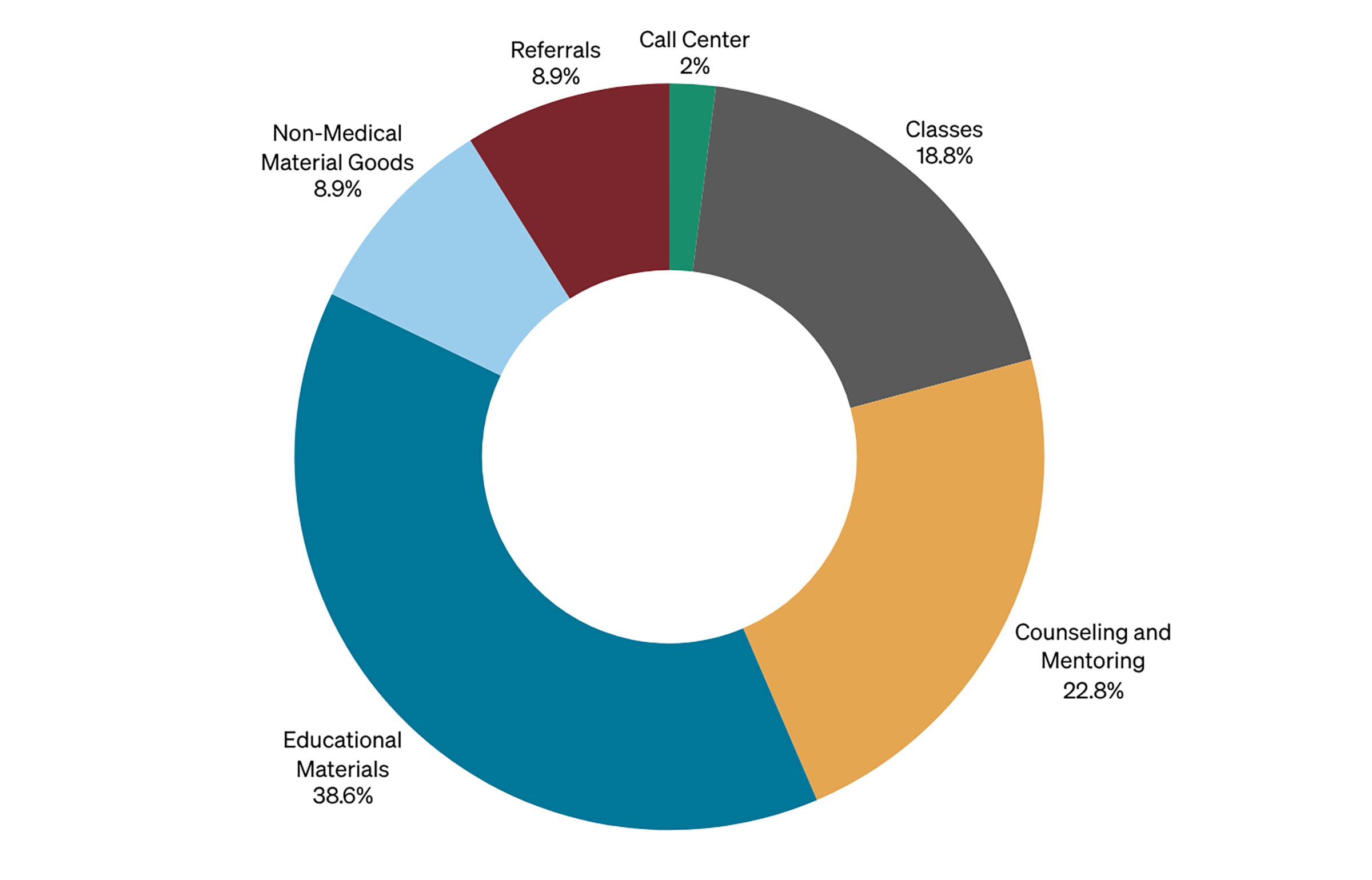
In FY24, TTF-funded organizations provided billable services in six categories, as noted in the program reports. State-published materials provide few definitions for these services, and no categories include medical services such as pregnancy tests, ultrasounds, or other prenatal care.
Educational materials (39%): These materials, such as pamphlets and hand-outs, focus on topics such as pregnancy, parenting, and adoption. The program guidance does not specify the content of the materials, and the state provides no oversight of their quality. Up until at least 2021, state guidance mandated that organizations provide “A Woman’s Right to Know,” the state anti-abortion pamphlet, which contains outdated and inaccurate medical information about abortion and childbirth.[24] Rather than prioritizing the distribution of such materials, leading infant and maternal health organizations emphasize more direct clinical and social support strategies as the most effective way to increase healthy pregnancies, childbirth, or parenting.[25]
Counseling and mentoring services (23%): These services may relate to pregnancy, education, parenting, adoption, life skills, or employment readiness. Despite use of the term “counseling,” there is currently no publicly available training or licensing requirement for staff or volunteers who provide these services.[26] This is a missed opportunity: 7% of maternal deaths in Texas in 2020 were attributed to mental health conditions, and the state’s own 2024 report on maternal mortality describes 100% of them as preventable.[27] The state’s Maternal Mortality and Morbidity Review Committee (MMMRC) recommends as a solution that “providers should be trained on appropriate screening, diagnosis, referral, and treatment for perinatal mood and anxiety disorders,” suggesting these services would be better provided by licensed providers.[28]
Classes (19%): Specific topics for classes are not mandated but may include parenting, life skills, employment support, and educational attainment; curricula need not be evaluated by TTF or the state.[29] TTF does not impose training or certification requirements for class teachers or facilitators, and research shows this type of class is often faith-based.[30]
Non-medical material goods (9%): These goods must “directly support or promote childbirth” and may include items such as maternity clothes, car seats, or diapers.[31] TTF does not report details about goods provided or the quantification of a “good” (i.e., a single diaper versus a pack of diapers). Although providing material goods offers practical support, according to prior findings such aid is typically limited and distributed only in exchange for participating in program classes.[32]
Referrals to programs (9%): Although not all referrals result in program enrollment, these referrals provide linkages to programs such as Medicaid, the Supplementary Nutrition Assistance Program (SNAP), or Nurse Family Partnership (NFP), as well as other government assistance programs for housing, childcare, and transit.[33] However, the TTF report lacks data on client enrollment numbers, and rates vary significantly, making actual program uptake difficult to measure.
Call center (2%): Although the 2024 program documents do not define call center services, previous A2A and TTF documentation suggests that call centers provide information about TTF-funded organization services and schedule appointments for services such as lay counseling at TTF-funded sites, as described above.[34]
Other services: Finally, the FY24 TTF report also lists “care coordination for prenatal, perinatal, and postnatal services, including connecting participants to health services” and “housing services” as funded activities, but does not document any information about what these services include, their frequency, or any overlap with the services listed above.[35] Because Medicaid now pays for care coordination for pregnant members, these services could be more effectively delivered through patients’ existing health care providers.
Figure 2 — 2024 TTF Funded Services
Geographic Funding Disparities
Funding allocation by health service region (HSR) was determined using the FY24 list of non-virtual locations. For organizations with multiple sites, awards were divided equally among locations. This method was adopted because TTF does not report client numbers or service provision at the HSR level.
TTF funding was not distributed to HSRs in proportion to the population of reproductive-aged women, and the geographic criteria for these allocations remain unclear.[36] Key findings from the FY24 analysis include:
- Regional concentration: Two-thirds of the state’s regionally allocated funding was concentrated in just two HSRs.
- Northwest Texas/Metroplex saturation: Nearly half of all such funding went to just one region: HSR 2/3 (Dallas-Fort Worth and surrounding area).
- Gulf Coast/Southeast Texas gap: Despite having a similarly sized population of reproductive-aged women, HSR 6/5S (Houston and surrounding area) received just 12% of regionally allocated TTF funding, the lowest amount of funding per woman of reproductive age of any HSR.
Figure 3 — Geographic Distribution of TTF Funding Across Texas Health Service Regions (HSR)
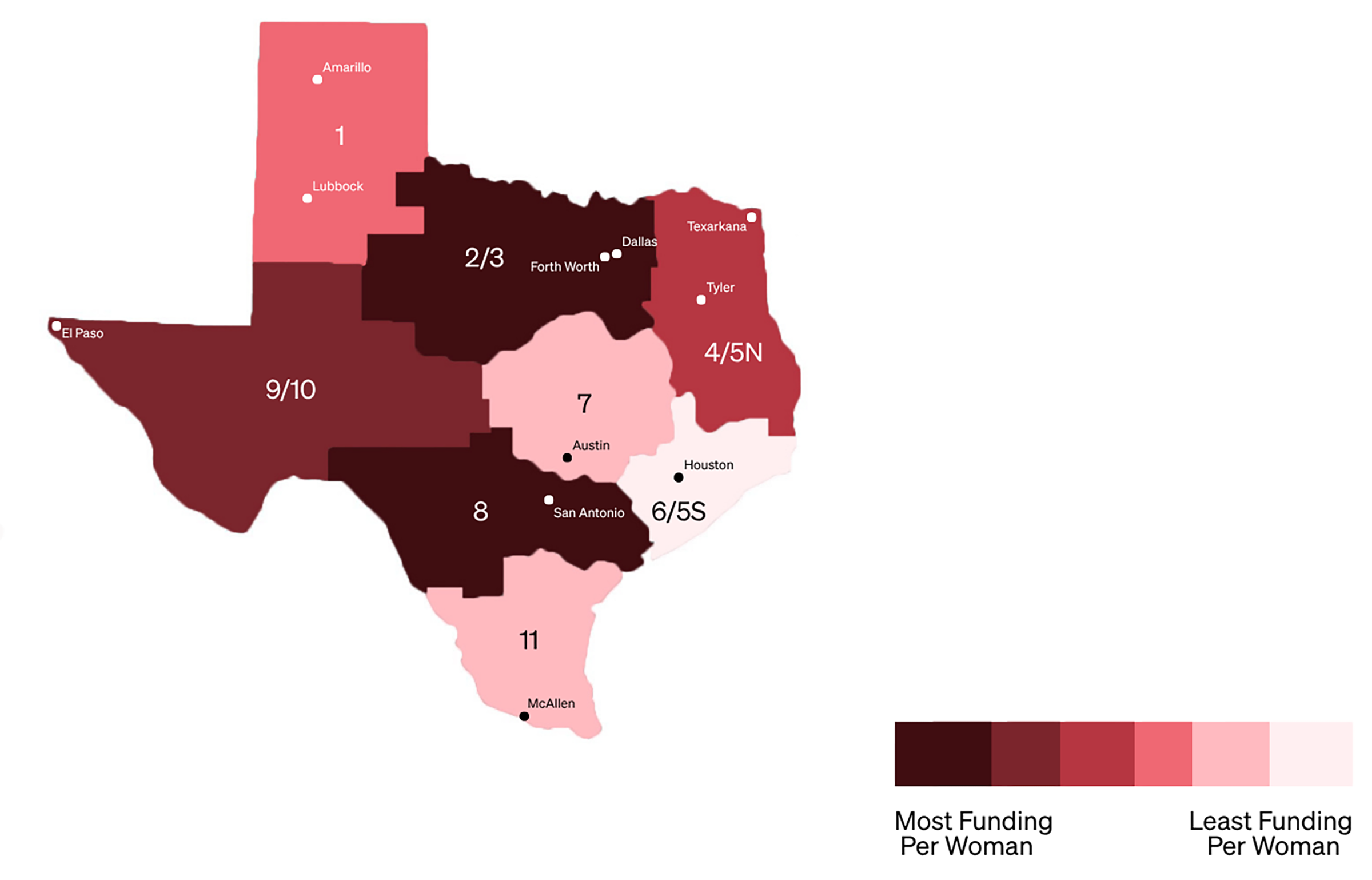
Table 3 — 2024 TTF Funding Distribution by HSR Relative to Population of Reproductive-Aged Women
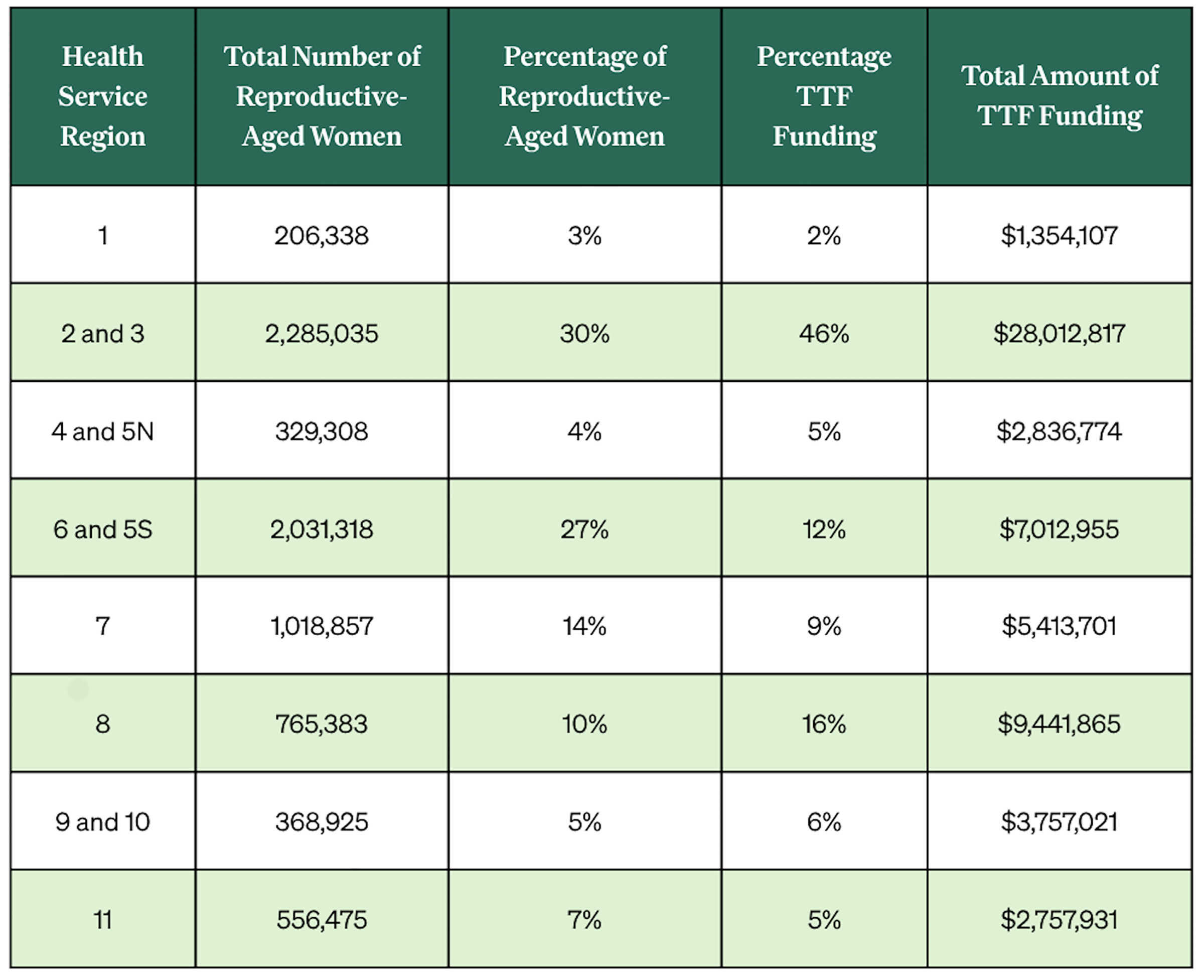
Source: Population estimates for 2024 sourced from the Texas Demographic Center; county-level HSR information from Texas Health and Human Services.
Note: Percentages may not total 100% due to rounding.
Evidence-Based Policy Solutions
The Texas Legislature has invested more in TTF than any comparable state program in the country. Despite this funding, there is little evidence to suggest TTF’s current contractors, strategies, or geographic distribution will effectively meet the program’s stated goals.[38]
While TTF focuses exclusively on non-medical support, many Texans currently lack access to basic health care services.[39] In addition to high rates of uninsured women of reproductive age and women with unmet contraceptive preferences, for instance, Texas’ maternal mortality rate — which falls disproportionately on people who are Black and living on low incomes — is considerably above the national average, and the state categorizes the vast majority of these deaths as preventable.[40]
To address these challenges, the following evidence-based policy shifts are recommended:
Invest in Existing Evidence-Based Programs
Expanding support for proven programs can directly improve maternal and infant health outcomes. Texas should prioritize investment in established state and federal programs, such as WIC (the Women, Infants, and Children program), which provides formula for eligible families along with breastfeeding support.[41] Similarly Medicaid, the Children’s Health Insurance Program, or state-specific programs with broad eligibility could provide diapers and similar items on a larger scale, mirroring successful models in other states.[42]
Texas also operates family support programs such as the Texas Nurse-Family Partnership program (NFP) that are aimed at supporting healthy parenting, infancy, and childhood.[43] By providing one-on-one home nursing visits during the first two years of parenthood, this program builds parenting skills.[44] Directing resources toward these and other evidence-based strategies would more effectively work toward the state’s goals of healthy pregnancies and child development.
Expand Health Care Coverage
Texas recently acknowledged the importance of safety-net coverage by extending postpartum Medicaid to 12 months. Despite the availability of federal matching funds for full-benefit Medicaid expansion to cover most adults with incomes below 138% of the federal poverty level (FPL), however, Texas is one of only 10 states to reject full-benefit Medicaid expansion.[45] By not expanding such coverage, the state continues to forgo significant federal matching funds. The state’s current income cutoff of 15% FPL for parents — less than $350 per month for a single parent of two children — is the lowest in the nation.[46]
If Texas were to expand Medicaid eligibility, work requirements would be obligatory as of January 2027, due to federal changes. Texas could minimize negative effects on recipients by avoiding the burdensome administrative procedures adopted in other states, such as excessive eligibility reverifications.[47]
Expanding Medicaid eligibility would enable many more Texans to access contraceptive methods, preconception care, and other preventive services such as annual exams and blood pressure screening. Such access would directly support the goals the state hopes to achieve through TTF, including healthier pregnancies and deliveries.
Shore Up the Provider Safety Net
Expanding the safety-net provider network would help to ensure that Texans enter pregnancy healthy and receive consistent care through the postpartum period.[48] As part of this, Texas should increase reimbursement rates under Medicaid and state-funded reproductive health programs, helping rural hospitals stay open and preventing further maternity care deserts.[49] Additionally, ending the exclusion of Planned Parenthood from Medicaid and state programs would support access to much-needed reproductive health care for the state’s most vulnerable populations.
Texas should also invest in the prenatal care infrastructure by expanding the maternal health care workforce, including nurse practitioners, certified nurse midwives, and doulas. Further, the state should modify financial incentives, such as the Rural Communities Health Care Investment Program, to include prenatal care.[50]
To help address health care deserts, the state has implemented a mobile health unit program that brings health care providers to rural areas at regular intervals.[51] While these units currently connect rural residents to obstetric care providers, expanding their scope and funding to include regular prenatal services would significantly improve maternal health access in underserved rural areas.
Conclusion
Texas’ record-high investment in TTF currently funds services with little oversight or demonstrated efficacy. To better serve the public interest, the state should shift its focus toward proven infrastructure and clinical care programs that directly address the state’s most pressing reproductive health needs.
Notes
[1] Texas Health and Human Services, Thriving Texas Families Report for Fiscal Year 2024, December 2024, https://www.hhs.texas.gov/sites/default/files/documents/thriving-texas-families-report-fy2024.pdf; Conference Committee, “General Appropriations Act for the 2026–27 Biennium,” 89th Leg., Reg. Sess. (Tex. 2025), https://www.lbb.texas.gov/Documents/GAA/General_Appropriations_Act_2026_2027.pdf; and H.B. 500, 89th Leg., Reg. Sess. (Tex. 2025), https://capitol.texas.gov/tlodocs/89R/billtext/html/HB00500F.htm.
[2] Thriving Texas Families Report for Fiscal Year 2024.
[3] “General Appropriations Act for the 2026–27 Biennium”; H.B. 500 (2025), https://capitol.texas.gov/tlodocs/89R/billtext/html/HB00500F.htm.
[4] “General Appropriations Act for the 2026–27 Biennium”; H.B. 500 (2025); and Executive Office of the Governor, “Governor Ron DeSantis Signs Florida Fiscal Year 2025–2026 Budget,” press release, June 30, 2025, https://www.flgov.com/eog/news/press/2025/governor-ron-desantis-signs-florida-fiscal-year-2025-2026-budget.
[5] Thriving Texas Families Report for Fiscal Year 2024; General Appropriations Act for the 2026–27 Biennium”; and H.B. 500 (2025).
[6] Elizabeth Sepper et al., “After Roe: Criminal Abortion Bans in Texas,” Texas Policy Evaluation Project, June 2022, https://sites.utexas.edu/txpep/files/2022/06/TexasPostRoeCriminalAbortionBans-TxPEP-PolicyBrief_27June22.pdf.
[7] Passed in 2023, Texas S.B. 24 (2023) codified and rebranded the Alternatives to Abortion program into the Thriving Texas Families program. Gracia Sierra et al., “Barriers to Preferred Contraceptive Use in Texas,” Rice University’s Baker Institute for Public Policy, November 4, 2025, https://www.bakerinstitute.org/research/barriers-preferred-contraceptive-use-texas; “March of Dimes Report Card,” March of Dimes, 2025, accessed February 4, 2026, https://www.marchofdimes.org/reportcard; National Center for Health Statistics (NCHS), “Maternal Deaths and Mortality Rates: Each State, the District of Columbia, United States, 2018–22,” Centers for Disease Control and Prevention (CDC), accessed January 23, 2026, https://www.cdc.gov/nchs/maternal-mortality/MMR-2018-2022-State-Data.pdf; “Birth Demographics,” Texas Health Data, Texas Health and Human Services, accessed February 10, 2026, https://healthdata.dshs.texas.gov/dashboard/maternal-and-child-health/infant-health/birth-demographics; and NCHS, Teen Births: Birth Data Maps,” CDC, August 20, 2025, https://www.cdc.gov/nchs/state-stats/births/teen-births.html?CDC_AAref_Val=https://www.cdc.gov/nchs/pressroom/sosmap/teen-births/teenbirths.htm.
[8] “Health Insurance Coverage By State,” National Women’s Law Center, April 30, 2025, https://nwlc.org/resource/health-insurance-coverage-by-state/.
[9] Texas Health and Human Services, Thriving Texas Families Report for Fiscal Year 2025, December 2025, https://www.hhs.texas.gov/sites/default/files/documents/thriving-texas-families-report-fy2025.pdf; S.B. 24, 88th Leg., Reg. Sess. (Tex. 2023), https://capitol.texas.gov/tlodocs/88R/billtext/html/SB00024F.htm.
[10] Texas Health and Human Services, “Request for Applications (RFA) For Alternatives to Abortion,” March 20, 2020, https://www.hhs.texas.gov/sites/default/files/documents/alternatives-abortion-fy2023-rider68.pdf.
[11] “Request for Applications (RFA) For Alternatives to Abortion.”
[12] S.B. 1388, 89th Leg., Reg. Sess. (Tex. 2025), https://capitol.texas.gov/tlodocs/89R/billtext/html/SB01388F.htm.
[13] S.B. 24 (2023); Jordan Smith, “No Real Alternative,” Austin Chronicle, January 26, 2007, https://www.austinchronicle.com/news/2007-01-26/439247/.
[14] “Request for Applications (RFA) For Alternatives to Abortion.”
[15] Thriving Texas Families Report for Fiscal Year 2024.
[16] Laura Dixon et al., “Texas’ Alternatives to Abortion Program: Historical Overview and Funding Analysis,” Resound Research for Reproductive Health, December 2024, https://resoundrh.org/wp-content/uploads/2025/03/ResoundRH-2024-A2A-1.pdf.
[17] Kendra Hutchens, “‘It Wasn’t Very Public-Clinicy’: Client Experiences at Faith-Based Pregnancy Centers,” Journal of Health and Social Behavior 64, no. 4 (2023): 486–502. https://dx.doi.org/10.1177/00221465231171555; Hutchens, “‘People Don’t Come in Asking for the Gospel, They Come In for a Pregnancy Test!’ Feminizing Evangelism in Crisis Pregnancy Centers,” Gender & Society 36, no. 2 (2022): 165–88, https://doi.org/10.1177/08912432211073061.
[18] Karan S. Desai et al., “Characterizing Services Advertised on Crisis Pregnancy Center Websites,” JAMA Internal Medicine 185, no. 2 (2025): 238–40. https://dx.doi.org/10.1001/jamainternmed.2024.6440; Amy G. Bryant and Jonas J. Swartz, “Why Crisis Pregnancy Centers Are Legal but Unethical,” AMA Journal of Ethics 20, no. 3 (2018): 269–77, https://dx.doi.org/10.1001/journalofethics.2018.20.3.pfor1-1803.
[19] “Why Crisis Pregnancy Centers Are Legal but Unethical”; Melissa N. Montoya et al., “The Problems with Crisis Pregnancy Centers: Reviewing the Literature and Identifying New Directions for Future Research,” International Journal of Women’s Health 14 (2022): 757–63, https://dx.doi.org/10.2147/IJWH.S288861; and Corynne McSherry, “RE: Potentially Deceptive Privacy Practices of Crisis Pregnancy Centers,” Electronic Frontier Foundation (EFF), letter to Attorney General Ken Paxton, January 28, 2025, https://www.eff.org/files/2025/01/28/2025.01.28_letter_to_tx_ag_with_exhibits.pdf.
[20] Maria F. Gallo et al., “Contraception and Abortion Misinformation Among Crisis Pregnancy Center Attendees and Non-Attendees,” Contraception 156 (2026): 11321, https://www.contraceptionjournal.org/article/S0010-7824(25)00512-8/fulltext.
[21] “The Problems with Crisis Pregnancy Centers.”
[22] Katrina Kimport et al., “The Prevalence and Impacts of Crisis Pregnancy Center Visits Among a Population of Pregnant Women,” Contraception 98, no. 1 (2018): 69–73, https://dx.doi.org/10.1016/j.contraception.2018.02.016.
[23] Isacc Maddow-Zimet et al., “Monthly Abortion Provision Study,” Open Science Framework (OSF), updated March 23, 2026, https://dx.doi.org/10.17605/OSF.IO/K4X7T; Society of Family Planning, #WeCount Report, April 2022 Through December 2024, June 23, 2025. https://dx.doi.org/10.46621/725961gzsnai.
[24] “Request for Applications (RFA) For Alternatives to Abortion”; Daniel Grossman, “Grossman: State’s ‘Woman’s Right to Know’ Booklet Is Lacking,” Austin American-Statesman, September 15, 2016, https://www.statesman.com/story/news/2016/09/15/grossman-states-womans-right-to-know-booklet-is-lacking/10080118007/; Cynthia Daniels, “Texas 2019: Evaluation of Women’s Right to Know Brochure,” June 10, 2019, https://informedconsentproject.com/wp-content/uploads/2019/06/Texas-2019-State-Information-Sheet-FINAL-1.pdf.
[25] March of Dimes, “2025–2026 Policy Priorities,” January 2025, https://www.marchofdimes.org/sites/default/files/2025-01/2025_2026_OGA_Policy_Priorities.pdf; Prenatal-to-3 Policy Impact Center, “2025 Prenatal-to-3 State Policy Roadmap,” Vanderbilt University Peabody College of Education & Human Development, 2025, https://pn3policy.org/pn-3-state-policy-roadmap-2025/.
[26] “Request for Applications (RFA) For Alternatives to Abortion”; Texas Health and Human Services, “Thriving Texas Families,” accessed March 11, 2026, https://www.hhs.texas.gov/services/health/women-children/thriving-texas-families.
[27] Texas Human and Health Services, Texas Maternal Mortality and Morbidity Review Committee and Department of State Health Services Joint Biennial Report 2024, September 1, 2024, https://www.dshs.texas.gov/sites/default/files/legislative/2024-Reports/MMMRC-DSHS-Joint-Biennial-Report-2024.pdf.
[28] Texas Maternal Mortality and Morbidity Review.
[29] Thriving Texas Families Report for Fiscal Year 2024.
[30] “Health and Safety Code Title 2, Chapter 54,” Texas Constitution and Statutes, accessed January 21, 2026, https://statutes.capitol.texas.gov/?tab=1&code=HS&chapter=HS.54&artSec=; Sarah Butrymowicz and Caroline Preston, “They Just Tried to Scare Us’: Anti-Abortion Centers Teach Sex Ed Inside Some Texas Public Schools,” The Texas Tribune, October 2, 2023, https://www.texastribune.org/2023/10/02/crisis-pregnancy-centers-texas-sex-ed/; and Katrina Kimport, “Pregnant Women’s Experiences of Crisis Pregnancy Centers: When Abortion Stigmatization Succeeds and Fails,” Symbolic Interaction 42, no. 4 (2019): 618–39, https://dx.doi.org/10.1002/symb.418.
[31] “Request for Applications (RFA) For Alternatives to Abortion”; and Thriving Texas Families Report for Fiscal Year 2024.
[32] Alexandra Kissling et al., “Free, but at What Cost? How U.S. Crisis Pregnancy Centres Provide Services,” Culture, Health & Sexuality 25, no. 8 (2023): 1024–38. https://dx.doi.org/10.1080/13691058.2022.2116489; Cassandra Jaramillo et al., “Texas Sends Millions to Crisis Pregnancy Centers. It’s Meant to Help Needy Families, but No One Knows If It Works,” ProPublica and CBS News, July 9, 2024, https://www.propublica.org/article/texas-funding-anti-abortion-crisis-pregnancy-centers.
[33] Thriving Texas Families Report for Fiscal Year 2024.
[34] Thriving Texas Families Report for Fiscal Year 2024; “Request for Applications (RFA) For Alternatives to Abortion.”
[35] Thriving Texas Families Report for Fiscal Year 2024.
[36] Based on author’s analysis of it is based on your analysis of the Thriving Texas Families Report for Fiscal Year 2024.
[37] “Vintage 2024 Population Estimates,” Texas Demographic Center, accessed March 11, 2026, https://demographics.texas.gov/Estimates/; “Texas County Numbers and Public Health Regions,” Texas Department of State Health Services, accessed March 11, 2026, https://www.dshs.texas.gov/center-health-statistics/texas-county-numbers-public-health-regions.
[38] “Health and Safety Code Title 2, Chapter 54,” Texas Constitution and Statutes, accessed January 21, 2026, https://statutes.capitol.texas.gov/?tab=1&code=HS&chapter=HS.54&artSec=; Texas Health and Human Services, “Request for Applications (RFA) Grant for Thriving Texas Families Program Pilot Projects,” March 26, 2022, https://bit.ly/3QGc6Bm.
[39] “Prenatal, Delivery, and Postpartum Care,” Texas Health Data, accessed February 27, 2026, https://healthdata.dshs.texas.gov/dashboard/maternal-and-child-health/maternal-health/prenatal-delivery-and-postpartum-care.
[40] “Health Insurance Coverage By State,” National Women’s Law Center, April 30, 2025, https://nwlc.org/resource/health-insurance-coverage-by-state/; “Barriers to Preferred Contraceptive Use in Texas”; “Maternal Deaths and Mortality Rates”; and Texas Maternal Mortality and Morbidity Review.
[41] “About WIC,” Texas Health and Human Services, updated April 2, 2026, https://texaswic.org/about-wic.
[42] Massachusetts Association for Community Action, “Changing Diapers, Changing Lives,” September 2025, https://www.masscap.org/wp-content/uploads/2025/09/MASSCAP-CHW-Diaper-Pilot-Program-Report-2025.pdf; American Hospital Association, “Delaware, Tennessee become first states to provide diapers through Medicaid,” May 22, 2024, https://www.aha.org/news/headline/2024-05-22-delaware-tennessee-become-first-states-provide-diapers-through-medicaid.
[43] Texas Health and Human Services, “Family Support Programs,” updated March 31, 2026, https://fss.hhs.texas.gov/family-support-programs.
[44] Texas Health and Human Services, “Texas Nurse-Family Partnership,” updated March 31, 2026, https://fss.hhs.texas.gov/programs/texas-nurse-family-partnership.
[45] KFF, “Status of State Medicaid Expansion Decisions,” March 12, 2026, https://www.kff.org/medicaid/status-of-state-medicaid-expansion-decisions/.
[46] KFF, “Medicaid Income Eligibility Limits for Adults as a Percent of the Federal Poverty Level,” January 2025,https://www.kff.org/affordable-care-act/state-indicator/medicaid-income-eligibility-limits-for-adults-as-a-percent-of-the-federal-poverty-level/.
[47] Akeiisa Coleman and Sara Federman, “Work Requirements for Medicaid Enrollees,” The Commonwealth Fund, September 30, 2025, https://www.commonwealthfund.org/publications/explainer/2025/sep/work-requirements-medicaid-enrollees.
[48] Jazmin Fontenot et al., “Where you Live Matters: Maternity Care Desserts and the Crisis of Access and Equity in Texas,” March of Dimes, 2023, https://www.marchofdimes.org/peristats/assets/s3/reports/mcd/Maternity-Care-Report-Texas.pdf.
[49] Kaitlin Berns et al., Maternity and Perinatal Care Deserts: A Report of the Texas Research-to-Policy Collaboration Project, September 11, 2024, https://bit.ly/48nqF2V.
[50] Texas Department of Agriculture, “Rural Communities Health Care Investment Program,” March 3, 2026, https://texasagriculture.gov/Grants-Services/RCHIP.
[51] Texas Women’s Healthcare Coalition, “Women’s Health on Wheels: Mobile Health Unit Brings Care to Women’s Healthcare Deserts,” November 11, 2025, https://www.texaswhc.org/stories/mhu-whow/.
This publication was produced by Rice University’s Baker Institute for Public Policy. Wherever feasible, the material was reviewed by outside experts prior to release. Any errors or omissions are solely the responsibility of the author(s).
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author(s) and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s) and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.


