
Executive Summary
When women can use their preferred contraceptive method, they are more likely to use it consistently, supporting their family formation and other life goals. Inequities in contraceptive access undermine reproductive autonomy, deepen health disparities, and contribute to higher rates of unwanted pregnancy and adverse maternal outcomes across the state. In Texas, where women face substantial logistical and financial barriers to ending an unwanted pregnancy, ensuring access to preferred contraceptive methods is more critical than ever.[1]
Despite changes in state policies and funding over the past decade aimed at restoring access to family planning services after cuts made by the legislature, many Texans still do not use their preferred contraceptive methods. This report examines contraceptive use from 2014 to 2023, trends in unmet preferences, and barriers to reproductive health care by insurance status, with the aim of informing policy solutions to improve access across the state.
Background
In 2011, Texas reduced funding for its family planning safety net by two-thirds and excluded Planned Parenthood, the state’s largest provider, from state-funded programs. These changes led to clinic closures and loss of access to essential reproductive health services, including contraception, sexually transmitted infection (STI) testing and treatment, and screening for reproductive cancers, for thousands of low-income residents.[2] Between 2013 and 2016, the state reallocated resources to the family planning budget and established new programs to restore access to reproductive health care for Texans living on low incomes. However, Planned Parenthood remains excluded from these programs. Additionally, Texas has not expanded Medicaid and 23% of reproductive-aged women (18–45) are uninsured — the highest percentage in the nation.[3]
These changes in the policy and service landscape over the last decade have created persistent gaps in coverage and service availability making it difficult for Texans — particularly those who are uninsured or using public insurance — to access contraception in general and their preferred method in particular. Challenges accessing care fall most heavily on structurally disadvantaged communities, including lower income, rural, and non-English speaking Texans who are also more likely to be uninsured or publicly insured.[4]
This report examines Texas women’s patterns of contraceptive use and trends in use of their preferred method — a critical indicator of reproductive autonomy and reflection of how well the health care system makes the contraceptive options they want to use affordable and accessible.[5] Drawing on data from three statewide surveys of Texas women aged 18–49, the research assesses how the share of reproductive-aged Texans using their preferred contraceptive method has changed over time.[6] This analysis also details variation by insurance status:
- Private Insurance — Health coverage obtained either through an employer (employer-sponsored health plan) or purchased directly by an individual on the health insurance marketplace. These plans typically require the individual to pay premiums, deductibles, and co-pays.
- Public Insurance — Primarily for low-income Texans, this includes full-benefit Medicaid health insurance, and programs such as Healthy Texas Women (HTW) — a Medicaid program delivering select family planning and reproductive health services to women who meet eligibility criteria. In addition, this group includes local hospital and county-funded programs that cover family planning services for low-income Texans ineligible for other coverage.[7]
- No Insurance — Individuals who do not have any form of coverage. These Texans must cover the full cost of health care services, including contraception, out-of-pocket. They may be able to obtain family planning and preventive health services at low or no cost at health centers that receive funding from the federally funded Title X Family Planning Program and/or state-funded Family Planning Program.
These three categories align with those used in prior Resound research to maintain comparability and consistency over time. The insurance status of survey participants was determined by their answer to this question: “What type of health insurance do you have right now to help pay for birth control methods or other reproductive health care services?”
Methodology
Three representative statewide surveys were conducted in 2014, 2019, and 2023 using the Ipsos KnowledgePanel, among Texas women — or individuals assigned female at birth — aged 18–49.[8] Participants completed online surveys that assessed their contraceptive use and preferences, as well as access to family planning services. Responses were weighted to reflect the state’s demographic profile.
The analysis for this report was structured as follows:
Sample Selection Criteria — The study sample was limited to women aged 18–49 who were not pregnant, not trying to become pregnant, had ever had sex with men, and who reported both current and preferred contraceptive methods.
Current Method Analysis — Analyses of current contraceptive method use included 1,870 women (592 in 2014, 666 in 2019, and 612 in 2023).
Preferred Method Analysis — For analyses of preferred method, unmet preference, and barriers to access, women who were currently using permanent methods were excluded. This yielded a final sample of 1,288 women were included (382 in 2014, 478 in 2019, and 428 in 2023).
Statistical Testing — Chi-squared tests were used to assess differences over time and across groups. Only comparisons that were statistically significant (p<0.05) were reported.[9]
Main Findings
1. Half of Reproductive-Aged Texas Women Do Not Use Their Preferred Contraceptive Method
With 85% of reproductive-aged Texans reporting contraceptive use in 2023, the breakdown reveals reliance on the following types:
- Less Effective — 36% relied on methods that do not require a visit to a health care provider and are typically less effective at preventing pregnancy, such as fertility awareness, condoms, withdrawal, and breastfeeding.
- Permanent — 35% were using a permanent method, including tubal sterilization or vasectomy.
- Long-Acting Reversible — 14% were using intrauterine devices (IUDs) or contraceptive implants, collectively referred to as long-acting reversible contraceptives (LARC).
- Short-Acting —14% reported using short-acting hormonal methods, such as oral contraceptives, injectable contraception, patch, or vaginal ring.
The 2023 usage and distribution patterns were similar to those found in 2014 and 2019.
Despite a high prevalence of contraceptive use, over 50% of women reported having an unmet contraceptive preference — meaning they wanted to use a different method than the one they were currently using or wanted to start using a method if they were not already doing so. Importantly, this figure has remained largely unchanged for nearly a decade (Figure 1).
In all three surveys, those not currently using a method were the most likely to have an unmet preference, and approximately 90% of Texans in 2023 who were not using contraception wanted to. Among Texans who were using a method, 46% had an unmet preference, and nearly two-thirds of the women in this group relied on less effective methods, such as condoms and withdrawal.
Figure 1 — Just Over Half of Texas Women* Are Not Using Their Preferred Contraceptive Method
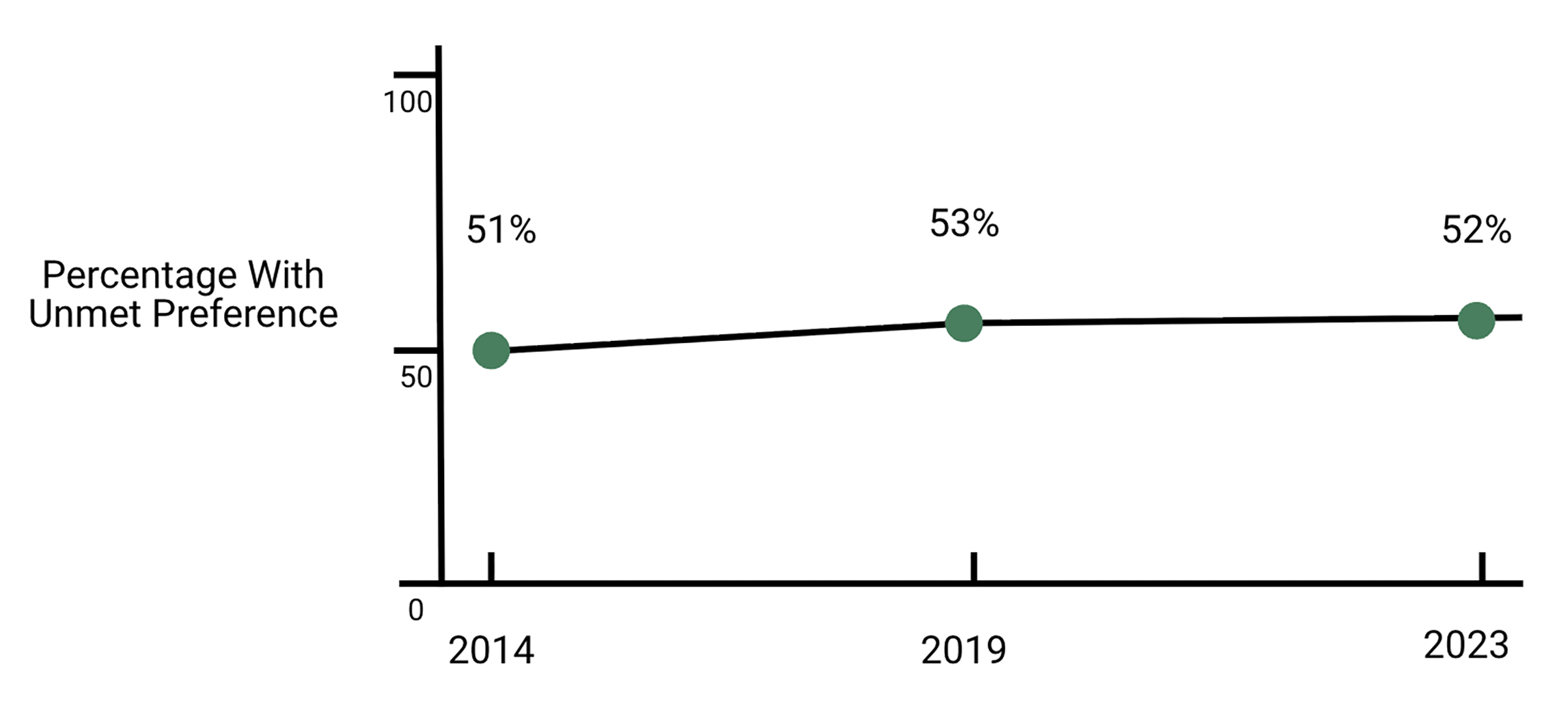
Note: *Texas women and residents assigned female at birth, between the ages of 18–49, who were not pregnant, not trying to become pregnant, and had ever had sex with a male partner.
2. Uninsured and Publicly Insured Women Are Less Likely to Use Preferred Contraception
In all survey years, uninsured and publicly insured women were more likely to have an unmet preference than those with private insurance. In 2023, 55% of uninsured and 59% of publicly insured women were not using their preferred contraceptive method. This was significantly higher than the 49% of privately insured women who had an unmet preference (Figure 2).
Figure 2 — Unmet Contraceptive Preference Is Higher Among Texas Women Than the National Average
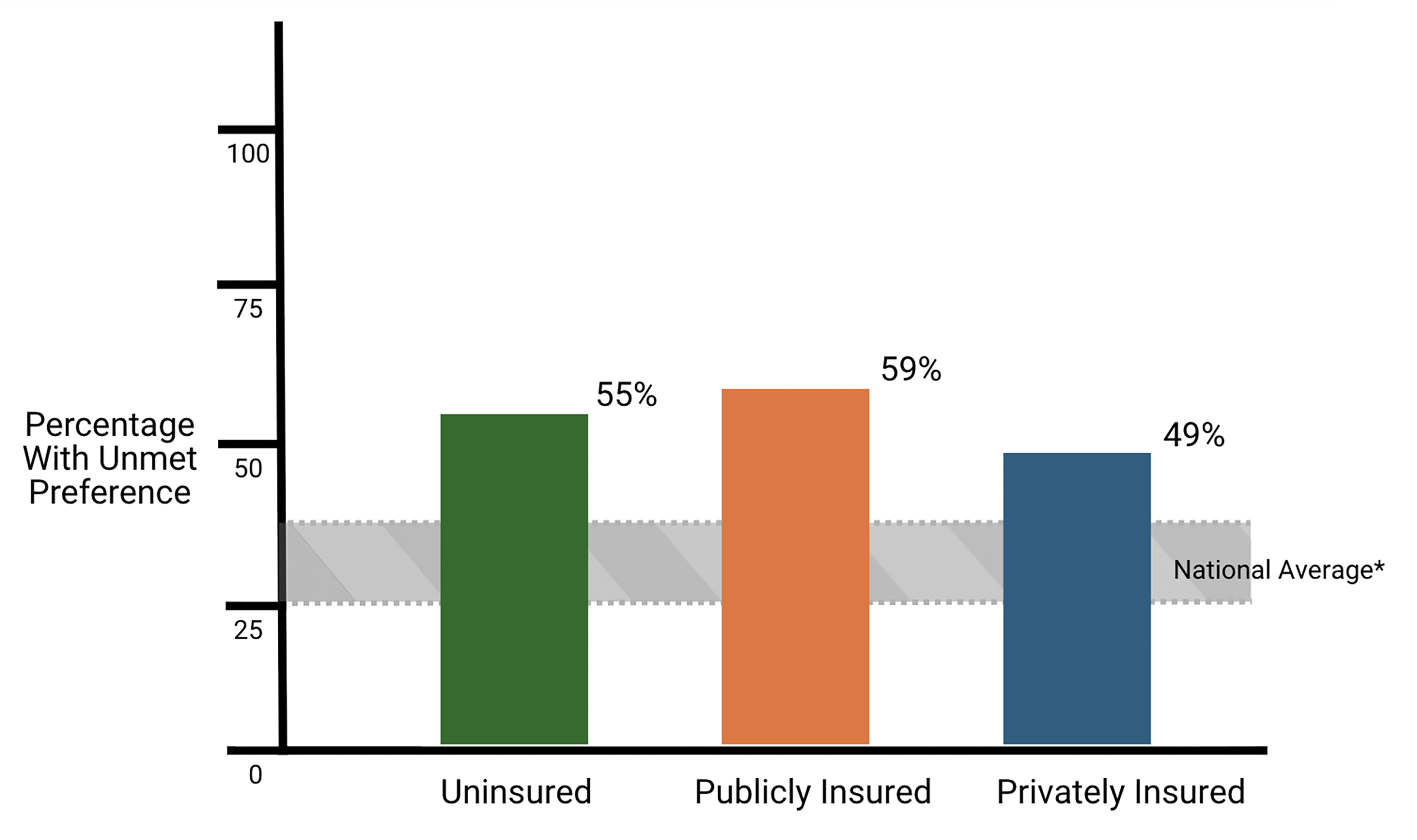
Note: Studies estimate the national range of unmet contraceptive preference from 25%–39%.
Among those with an unmet preference in 2023, permanent contraceptive methods were most commonly preferred. Approximately 1 in 3 Texan women with an unmet preference — regardless of insurance status — wanted permanent contraception, particularly tubal sterilization. Additionally, 1 in 4 (27%) publicly insured women with an unmet preference wanted to use a long-acting method instead of the method they were currently using. One in 6 uninsured and publicly insured women preferred to use short-acting hormonal contraceptives.
Notably, more than one-third (37%) of uninsured women did not express a preference for a specific method. This group largely consisted of people who had a high school diploma (65%), were not U.S.-born (49%), had a household income less than 100% of the federal poverty level (48%), and had not used health services in the last three years (88%) — all characteristics that may indicate limited access to information about the options that are available to them.
3. Insurance Gaps Create Persistent Barriers to Reproductive Health Care in Texas
Texans who were not using their preferred method often reported experiencing multiple barriers accessing reproductive health care. In 2023, 30% of women reported experiencing three or more barriers accessing care in the three years prior to the survey, but uninsured and publicly insured Texans were the most likely to report this: 50% of uninsured women and 37% of publicly insured women experienced more than three barriers to care, compared to only 20% of privately insured Texans.
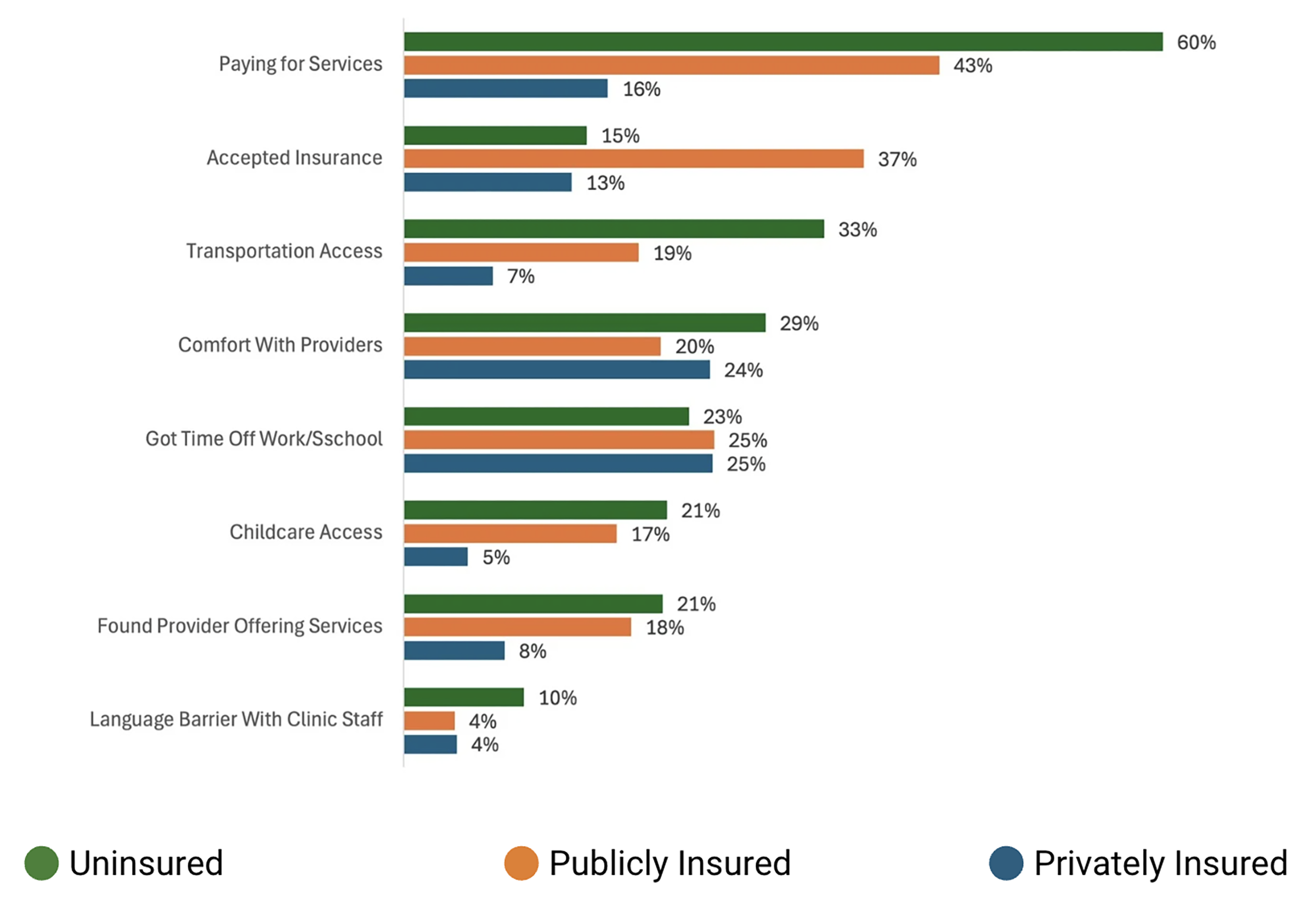
Across all survey years, Texans who were not using their preferred contraceptive method reported the same barriers accessing sexual and reproductive health care, but the specific barriers differed by insurance status.
- Affordability – Being unable to pay for services was the leading barrier for both uninsured (60%) and publicly insured women (43%), compared with only 16% of privately insured women (Figure 3).
- Provider Availability — Nearly 40% of publicly insured women also cited difficulty finding a provider or clinic that accepted their insurance.
- Logistical Challenges – Logistical challenges, such as getting transportation, time off work or school, and child care, were also common among uninsured and publicly insured women.
- Scheduling/Comfort – In contrast, privately insured women were more likely to report barriers related to provider comfort and scheduling rather than affordability or access.
Figure 3 — Barriers To Accessing Contraceptive Care Among Texas Women Not Using Their Preferred Method: By Insurance Status
Policy Recommendations
The prevalence of unmet contraceptive preference in Texas — even among those currently using a method — exceeds national estimates, where one quarter of women are not using their preferred method. The percentage of Texans with an unmet contraceptive preference is also higher than those reported for reproductive-aged women living in states that have diverse contraceptive access policies: Arizona (25%), Iowa (17%), New Jersey (26%), Mississippi (39%), Ohio (25%), and Wisconsin (33%).[11] With the exception of Mississippi, these states have broader contraceptive access policies, including Medicaid expansion (Iowa, New Jersey, Ohio, and Arizona), partial expansion and higher program eligibility (Wisconsin), and over-the-counter contraceptive access without a prescription.
These findings underscore the structural shortcomings that limit Texans’ access to reproductive health care and reproductive autonomy. Three complementary strategies would make it possible for Texans to use their preferred method — particularly the permanent and long-acting types that many want but cannot afford, due to their higher upfront costs (Figure 4):
- Expand health care coverage.
- Increase public program provider networks.
- Strengthen the safety net.
Figure 4 — Texas Women’s* Contraceptive Use if All Used Their Preferred Method
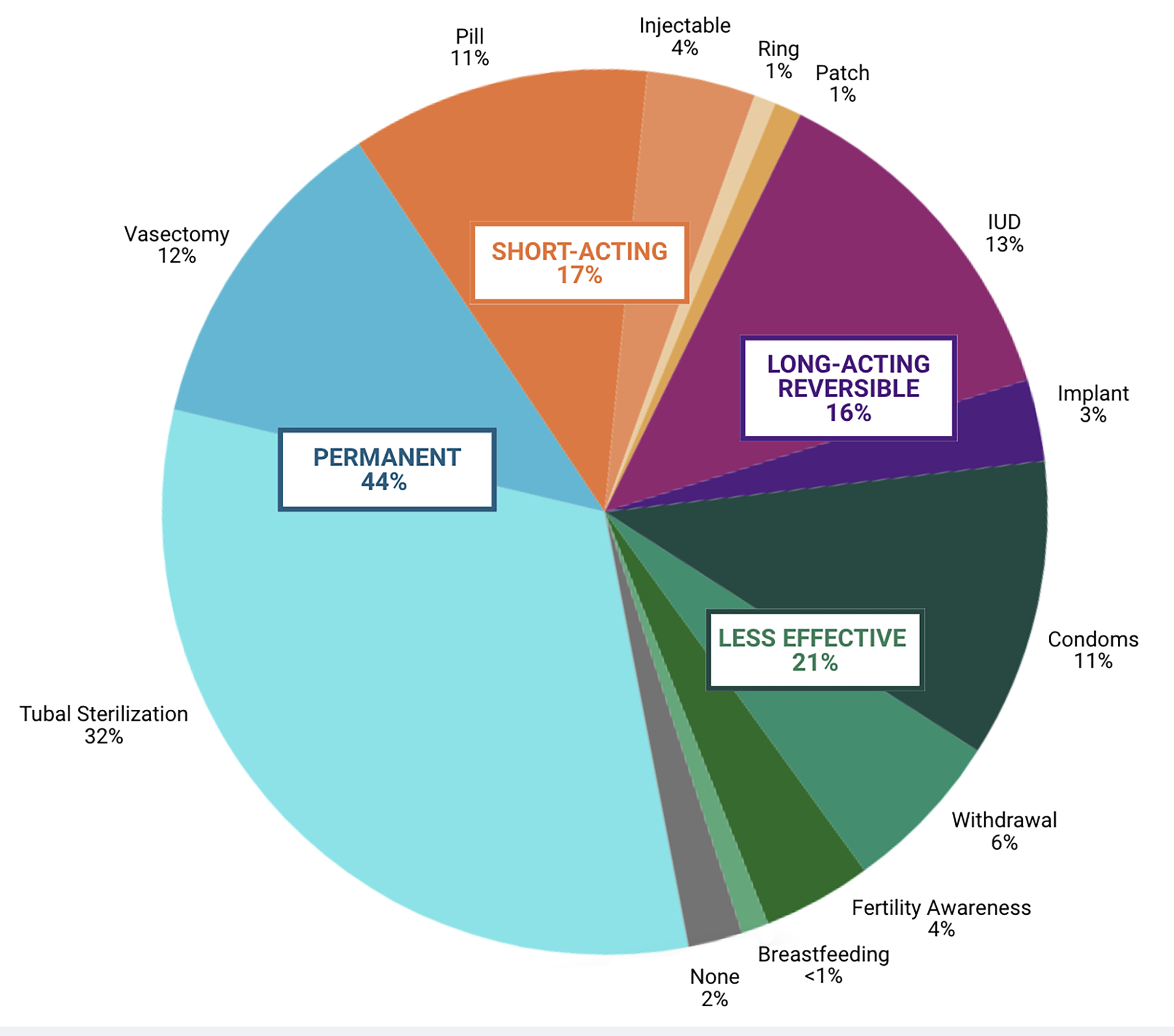
Note: *Numbers do not total 100 due to rounding. Respondents who answered, “Don’t know,” as well as missing respondents, are omitted.
1. Expand Health Care Coverage
A central policy priority should be expanding health care coverage to reduce the number of uninsured Texans. As one of just 10 states that has not expanded Medicaid under the Affordable Care Act (ACA), Texas could significantly improve access by pursuing two key paths: 1) expanding eligibility from 17% to 138% of the federal poverty level, and 2) streamlining enrollment through simpler applications, reduced paperwork, shorter processing times, and ensuring continuous coverage for people with fluctuating incomes.[12]
Marketplace coverage can also be strengthened through improved guidance, enrollment, and subsidies to make these plans more affordable and easier to use. Assistance from navigators or community organizations would also help those who are eligible obtain coverage.
2. Increase Public Program Provider Networks
To encourage more providers to participate in publicly funded programs, Texas could increase reimbursement rates and simplify administrative requirements. Expanding the number of participating providers who offer permanent contraception methods and who are trained in the insertion and removal of long-acting reversible contraceptives (IUDs and implants) would ensure that clinics can meet the high demand for these methods.
Evidence shows that Planned Parenthood affiliates are highly effective at helping patients overcome structural barriers to care and serve large numbers of patients seeking contraception, despite being currently excluded from all publicly funded programs in Texas.[13] Including affiliates again in the provider network would help more Texans — particularly those living on low incomes — obtain their preferred contraceptive method by increasing the number of health centers offering the full range of contraceptive options and reducing barriers such as long travel distances and limited appointment availability.
3. Strengthen the Safety Net
Even in the absence of the changes suggested above, Texas policymakers could focus on strengthening existing programs for low-income residents. Increased funding for current programs would allow the current network of providers to serve more people and ensure that all clinics provide the full range of contraceptive methods, thereby facilitating access to their preferred method. Resources could also help clinics stock the full range of reversible contraceptive methods on-site and provide same-day access, which is a best practice in contraceptive care. This would reduce common barriers — such as the need for multiple visits, out-of-pocket costs, transportation challenges, and getting time off work — that disproportionately affect Texans relying on publicly funded health programs or lacking coverage.
Additional funding could also allow clinics to offer extended hours — including evenings, weekends, and walk-in appointments — to accommodate those with limited flexibility with their work, school, or caregiving responsibilities. Funding could also improve online and mobile tools and support outreach through community-based organizations. These efforts could help Texans who are disconnected from care or uncertain about their options to locate clinics and make informed decisions about available contraceptive methods.
Notes
[1] Adam Sonfield, “Why Family Planning Policy and Practice Must Guarantee a True Choice of Contraceptive Methods,” Guttmacher Policy Review 20, November 1, 2017, https://www.guttmacher.org/gpr/2017/11/why-family-planning-policy-and-practice-must-guarantee-true-choice-contraceptive-methods.
[2] Emma Carpenter et al., “Publicly Funded Reproductive Health Care Programs for People with Low Incomes in Texas, 2011–2021,” Texas Policy Evaluation Project, The University of Texas at Austin, March 2021, https://resoundrh.org/wp-content/uploads/2024/11/txpep-2021-repro-health-programs-brief.pdf; Kari White et al., “The Impact of Reproductive Health Legislation on Family Planning Clinic Services in Texas,” American Journal of Public Health 105, no. 5 (2015): 851–8, https://pubmed.ncbi.nlm.nih.gov/25790404/.
[3] “Texas Women’s Health Insurance Coverage Data,” KFF, https://www.kff.org/interactive/womens-health-profiles/texas/healthcare-coverage/.
[4] Matthew Buettgens et al., The Uninsured in Texas: Statewide and Local Area Views, Urban Institute Health Policy Center, December 2018, https://www.urban.org/sites/default/files/publication/99498/uninsured_in_texas_2.pdf; Jennifer Tolbert et al., “Key Facts about the Uninsured Population,” KFF, December 18, 2024, https://www.kff.org/uninsured/key-facts-about-the-uninsured-population/.
[5] Joseph E. Potter et al., “Challenging Unintended Pregnancy as an Indicator of Reproductive Autonomy,” Contraception 100, no. 1 (2019): 1–4, https://dx.doi.org/10.1016/j.contraception.2019.02.005.
[6] In 2014 and 2019, the survey inclusion criteria was “women.” In 2023 it was “people assigned female at birth.”
[7] “Healthy Texas Women,” Texas Health and Human Services, https://www.healthytexaswomen.org/; Department of Health and Human Services Office of Population Affairs, “Title X Family Planning Program,” http://opa.hhs.gov/sites/default/files/2022-12/title-x-family-planning-program-2022.pdf.
[8] “KnowledgePanel,” Ipsos, https://www.ipsos.com/en-us/solutions/public-affairs/knowledgepanel.
[9] To perform Chi-Square tests, see: “The Chi-Square Test, JMP Statistical Discovery: Statistics Knowledge Portal,” https://www.jmp.com/en/statistics-knowledge-portal/chi-square-test.
[10] Amanda Nagle et al., “Barriers to Preferred Contraception Use in Mississippi,” Journal of Women’s Health 34, no. 2 (2025):198–205, https://dx.doi.org/10.1089/jwh.2024.0127; Brittni Frederiksen et al., “Contraception in the United States: A Closer Look at Experiences, Preferences, and Coverage,” KFF, November 3, 2022, https://www.kff.org/womens-health-policy/contraception-in-the-united-states-a-closer-look-at-experiences-preferences-and-coverage/; Megan L. Kavanaugh et al., “Associations Between Unfulfilled Contraceptive Preferences Due to Cost and Low-Income Patients’ Access to and Experiences of Contraceptive Care in the United States, 2015–2019,” Contraception: X 2022, no. 4 (2022): article 100076, https://doi.org/10.1016/j.conx.2022.100076; Payal Chakraborty et al., “Use of Nonpreferred Contraceptive Methods Among Women in Ohio,” Contraception 103, no. 5 (2021): 328–35, https://dx.doi.org/10.1016/j.contraception.2021.02.006; Laura E.T. Swan et al., “Exploring Financial Stress and Resource Deprivation as Barriers to Preferred Contraceptive Use in Wisconsin in 2021,” Contraception 115 (2022): 22–6, https://dx.doi.org/10.1016/j.contraception.2022.07.014; Kavanaugh et al., “Unfulfilled and Method-Specific Contraceptive Preferences Among Reproductive-Aged Contraceptive Users in Arizona, Iowa, New Jersey, and Wisconsin,” Health Services Research 59, no. 3 (2024): e14297, https://dx.doi.org/10.1111/1475-6773.14297.
[11] Nagle; Frederiksen; Kavanaugh, “Associations Between Unfulfilled Contraceptive Preferences”; Chakraborty; Swan; Kavanaugh, “Unfulfilled and Method-Specific Contraceptive Preferences”; and Whitney S. Rice et al. “Dispersion of Contraceptive Access Policies Across the United States From 2006 to 2021,” Preventive Medicine Reports 27 (2022):101827, https://dx.doi.org/10.1016/j.pmedr.2022.101827.
[12] Texas Women’s Healthcare Coalition, 89th Legislative Session Report, 2025, https://www.texaswhc.org/wp-content/uploads/2025/09/89th-Legislative-Report-Final-1.pdf; Every Body Texas, “A Brighter Texas for Everybody: 89th Legislative Agenda,” 2025, https://www.everybodytexas.org/uploads/files/general/EBTX-2025-Legislative-Priorities.pdf; and Every Body Texas, 2023 Legislative Report, 2023, https://www.everybodytexas.org/uploads/files/general/2023LegislativeReport.pdf.
[13] Amanda J. Stevenson et al., “Impact of Removal of Planned Parenthood from Texas Women’s Health Program,” New England Journal of Medicine 374, no. 9 (2016): 853–60, https://dx.doi.org/10.1056/NEJMsa1511902; “Effect of Removal of Planned Parenthood from the Texas Women's Health Program,” correction, New England Journal of Medicine 374, no. 13 (2016): 1298, https://dx.doi.org/10.1056/NEJMx160006; White et al., “The Risks of Excluding Qualified Family Planning Providers from Medicaid,” JAMA 334, no.10 (2025): 857–858, https://dx.doi.org/10.1001/jama.2025.12494; and Anna Chatillon et al., “Access to Care Following Planned Parenthood’s Termination from Texas’ Medicaid Network: A Qualitative Study,” Contraception 128 (2023): 110141, https://dx.doi.org/10.1016/j.contraception.2023.110141.
This publication was produced on behalf of Rice University’s Baker Institute for Public Policy. Wherever feasible, the material was reviewed by external experts prior to its release. Any errors are the responsibility of the author(s) alone.
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author(s) and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s) and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.


