
Overview
The 89th Texas Legislative Session demonstrated sustained interest in policies addressing non-medical drivers of health, which are the “conditions in the places where people live, learn, work, and play that affect a wide range of health risks and outcomes.” These legislative efforts centered on two key strategies: leveraging Medicaid’s In Lieu of Services authority to fund non-medical support and expanding provider types to deliver these services.
Two bills passed this session that address the health-related, non-medical needs of pregnant and postpartum Medicaid beneficiaries. These actions represent noteworthy progress for Medicaid policy and maternal health. They also laid important groundwork for the 90th legislative session to consider funding non-medical services for other priority health conditions and state health spending beyond the Medicaid program.
Proposed Legislation on Non-Medical Drivers of Health
In the 89th Texas legislative session, lawmakers introduced several proposals to fund services addressing the non-medical drivers of health (NMDOH). For this brief, NMDOH legislation is defined as bills funding non-medical services or providers to address health-related, non-medical needs of patients interacting with the health care delivery system. This analysis focuses on the NMDOH provisions of each bill; other details are not reflected in this brief.
In Lieu of Services
Six bills proposed leveraging the In Lieu of Services (ILOS) authority in Texas Medicaid (Table 1). Under ILOS, Medicaid managed care organizations (MCOs) can cover non-medical services that are medically appropriate and cost-effective substitutes for clinical care.
The Centers for Medicare and Medicaid Services (CMS) has issued guidance on using ILOS to address health-related, non-medical needs of beneficiaries. In Texas, the Health and Human Services Commission (HHSC) and the State Medicaid Managed Care Advisory Committee can approve a list of services that may be substituted for clinical care. These alternative services are optional; MCOs may choose whether or not to offer them, and beneficiaries may choose whether to participate in these services.
Currently in Texas, MCOs are already offering NMDOH interventions as value-added services, which are classified as an administrative cost (and excluded from capitation rate-setting). However, allowing coverage under ILOS is advantageous for budgeting because these costs are categorized as a medical expense, which counts toward the development of capitation rates and medical loss ratio.
In a presession policy report, “Enhancing Texas’ Health Care Investments by Addressing Patients’ Non-Medical Needs,” coauthors Elena M. Marks and Charles W. Mathias highlighted ILOS as a key funding mechanism for NMDOH services. Texas has previously exercised its ILOS authority: in 2019, SB 1177 authorized MCOs to offer interventions like crisis respite care in lieu of behavioral health services. Additionally, ten other states (California, Iowa, Kansas, Michigan, Minnesota, New Hampshire, New York, Oregon, Rhode Island, and Tennessee) already use ILOS for coverage of nutritional counseling and/or food provisions (e.g., food prescriptions, food-is-medicine).
The 89th session’s embrace of ILOS authority demonstrates an agile response to health care innovations for addressing health-related, non-medical needs. Compared to other funding mechanisms like Medicaid Section 1115 demonstration waivers, ILOS is an efficient process. For example, 1115 waivers, which are commonly used to cover non-medical services such as housing, food provisions, and employment supports, are more administratively complex, resource-intensive, and difficult to amend once approved. In the 88th session, a pilot project for food provision for pregnant and postpartum women was proposed for funding through a 1115 waiver (HB 2983 and SB 1675); while it passed the House, it failed to advance in the Senate.
Continued use of ILOS by the Texas Legislature is encouraged as an effective way to implement medically appropriate, cost-effective solutions for addressing health-related, non-medical needs that are the root cause of disease and disability.
Table 1 — In Lieu of Services Bills Arranged by Filing Date
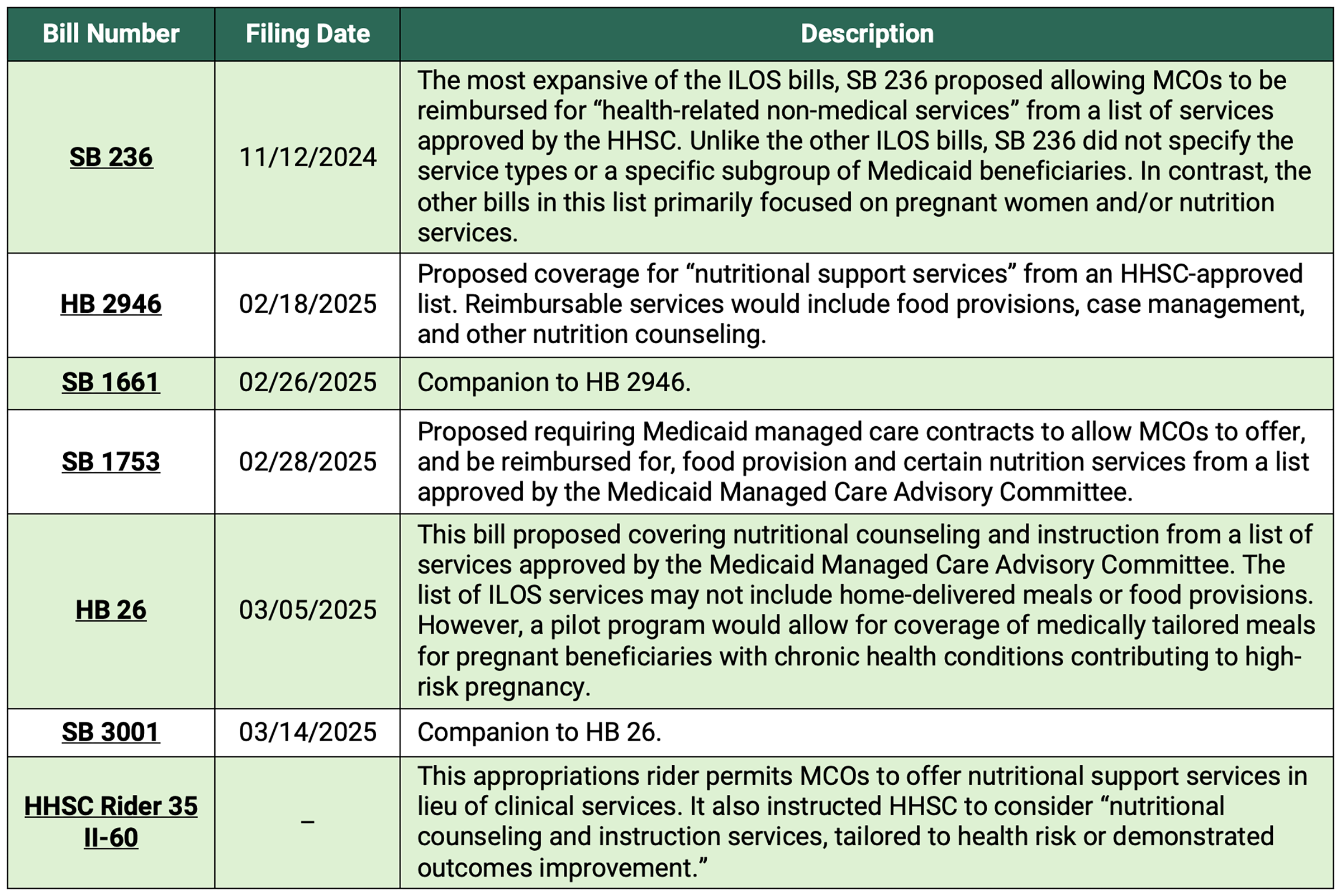
Of the six ILOS bills introduced, only HB 26 passed both chambers and was signed into law. It will take effect starting Sept. 1, 2025. The bill establishes a pilot program providing for medically tailored meals that runs through Sept. 1, 2031. At the program’s conclusion, HHSC will publish a report summarizing outcomes and recommendations for further policy action.
Debate Over Food Provision in Medicaid — As HB 26 moved through the legislative process, it underwent several amendments reflecting ongoing debate about the provision of food for a medical condition versus food insecurity. It is important to distinguish that Medicaid’s role in food provision coverage is to treat specific health conditions through clinically appropriate nutritional interventions, not to address food insecurity broadly. Programs such as the Supplemental Nutrition Assistance Program (SNAP) are designed to improve food access for low-income households, but are not structured as clinical tools for managing or treating disease.
HB 26 in the House — As initially filed, HB 26 explicitly excluded coverage for food provisions like home-delivered meals, food prescriptions, and grocery support. This exclusion was notable because coverage for food was the focus of the other ILOS bills (HB 2946, SB 1661, and SB 1753). The House later amended HB 26 by removing the food coverage exclusion and replacing it with language allowing “other nutrition support services provided to a recipient for a limited duration, as the commission determines, in coordination with nutrition counseling and instruction.” This revised language made food provision coverage a possibility.
HB 26 in the Senate — After the bill passed the House, the Senate restored the original exclusion of food provision coverage. In its place, senators added a pilot program to cover medically tailored meals for pregnant beneficiaries with chronic conditions such as gestational diabetes, hypertension, or obesity, which may contribute to high-risk pregnancies. During the floor debate, the rationale for adding the pilot program was described. It would enable more data to be gathered about health outcomes of food provisions for those with a priority health condition (pregnancy) before considering broader implementation for Medicaid beneficiaries with other health conditions. This emphasis on data collection is a step toward building the evidence base necessary to justify Medicaid coverage for non-medical services like medically tailored meals.
For the remaining five ILOS bills, all were referred to and left pending in committee.
In addition to the six ILOS bills, the budget bill — known as the General Appropriations bill SB 1 — included a rider addressing food provisions. The rider permits MCOs to provide nutritional support services using funds appropriated to HHSC. While this rider language does not specify whether medically tailored meals or other food provisions qualify as covered services, it recommends that HHSC consider the nutritional services, which are linked with health risks or demonstrated outcomes.
Non-Medical Maternal Health Workforce
The maternal health bills addressing NMDOH primarily focus on Medicaid coverage for new, non-medical provider types who can offer non-medical services.
Lactation Consultants — HB 136 authorizes Medicaid reimbursement for lactation consultants as a new provider type. This bill requires lactation consultants to hold certification from an international or national program approved by HHSC. Governor Abbott signed HB 136 into law, with an effective date of Sept. 1, 2025. Unlike the ILOS bills that were budget neutral, HB 136 carries a fiscal note, estimating $1,995,065 in two-year costs to cover an anticipated caseload of 54,861 recipients in fiscal year 2027. Sponsors noted the bill’s timeliness, as Medicaid postpartum coverage was extended from two to 12 months during the 88th session (HB 12), resulting in more breastfeeding mothers becoming enrolled in the Medicaid program. While not a clinical intervention, breast milk is an optimal food source for infant nutrition, and breastfeeding improves health for both infants and mothers.
Doula Services — Four bills proposed coverage of doula services. Doulas are trained and certified non-medical professionals who provide childbirth education and emotional and physical support during pregnancy, labor, delivery, and the post-partum period. Given their association with better maternal and infant outcomes, Medicaid coverage of doula services was proposed again this legislative session as a strategy to prevent pregnancy-related deaths and complications. This approach is consistent with recommendations from the Texas Maternal Mortality and Morbidity Review Committee and the Texas Department of State Health Services. More than 30 states have already implemented or are in the process of implementing laws to reimburse doula services through their Medicaid programs.
A pilot program (HB 1201) provided doula coverage of childbirth education, coaching, and support services throughout pregnancy and the postpartum period. Of the four doula bills, this one progressed the farthest, passing the House but stalling in the Senate Health and Human Services committee.
Other legislative approaches proposed funding doulas to provide non-medical support services, including:
- HB 3121 — Establish Medicaid coverage for doula services and reporting on the program’s performance.
- HB 5583 — Provide Medicaid coverage for doula support and case management.
- HB 2477 — Include coverage for doula support in the group health plans for governmental employees and retirees.
These other bills were referred to and left pending in committee.
Texas Information and Referral Network (2-1-1)
HB 38 proposed adding NMDOH screening for callers to the Texas Information and Referral Network 2-1-1 system. The bill would have required the use of a standard screening tool to identify non-medical needs of callers who provided consent to be screened, allowed data exchange with external partners to address NMDOH, and permitted data sharing with MCOs to address housing, transportation, food, and financial needs. Although HB 38 passed out of the House, it did not advance in the Senate.
Discussion
The 89th session continued the trend of proposing policies covering non-medical services to improve health outcomes in Texas. The success rate of NMDOH bills was 16.7% (2 passed of 12 filed), surpassing the overall session passage rate of 13.9% (1,213 passed, 8,719 filed).
The 88th session saw 11 bills introduced, but only one (HB 1575) was signed into law. Both the current and last sessions had significant activity around bills proposing coverage of doula services. However, the 89th session introduced a new and active approach leveraging ILOS in the state Medicaid program.
Despite this progress, NMDOH legislation remains narrow in scope, focusing on a limited range of specific services, conditions, and funding mechanisms. The bills passed into law from the 89th session:
- Targeted only a narrow set of non-medical services, such as nutrition support.
- Focused on a small set of priority health conditions like pregnancy.
- Concentrated on Medicaid as the primary funding mechanism for non-medical services.
Recommendations for the 90th Session
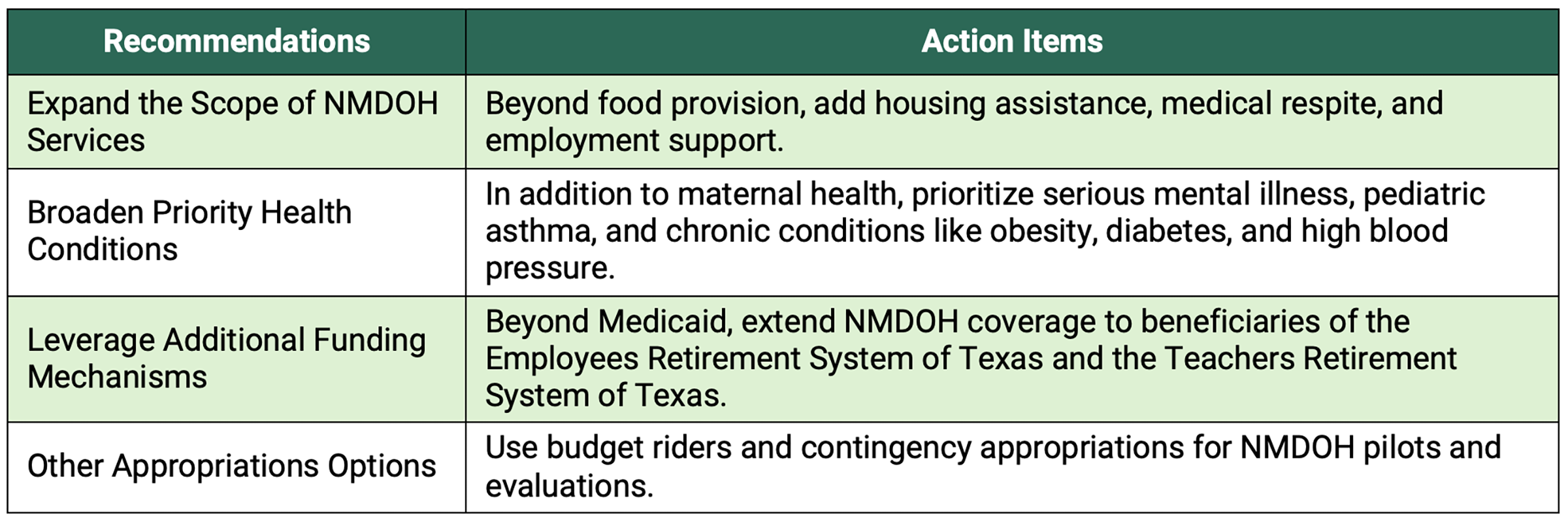
Building on the success of the 89th session, the legislature may consider closing gaps in scaling non-medical services. General principles for realizing the benefit of these services are outlined in Table 2.
Table 2 — Opportunities to Scale NMDOH Solutions for Texas
Considerations for the Biennium
Several important sources of evidence are expected during the biennium that may inform Texas policy on health-related, non-medical needs.
HB 1575: Maternal Health Outcomes Report
The health outcomes report required under HB 1575 (88th session) is anticipated in December 2026. This program standardizes screening for non-medical needs of pregnant and postpartum women in the Medicaid program and connects them to case management to address identified needs.
The report will provide:
- Prevalence of non-medical needs of women receiving case management.
- Number and types of referrals made for non-medical community assistance programs and providers.
- Birth outcomes for these women and their infants.
This analysis will help answer a critical question: What impact does addressing non-medical needs have on maternal and child outcomes? Findings will add to the evidence base supporting the value of non-medical services in health policy.
HB 1575: Early Implementation Findings
The initial HB 1575 report, published by HHSC in December 2024, documented early implementation. At that time, it was too early to report health outcomes linked to NMDOH screening and navigation. Instead, the report focused on developing the standardized screening tool and rates of prenatal risk factors for the Medicaid managed care pregnant population.
Key findings from the pilot of 1,156 participants identified rates of non-medical needs:
- 36% food insecurity.
- 21% child-care needs.
- 13% housing quality issues.
- 13% utility assistance.
Notably, while food, housing, and transportation are priorities in the HHSC NMDOH Action Plan, child care is not currently included. However, among women reporting child-care needs in the HB 1575 pilot program, 84% expressed interest in receiving services, a higher rate than even interest in food assistance (66% rate). This data presents an opportunity for HHSC to consider priorities for subgroups of the Medicaid population —like pregnant and postpartum women — in the next iteration of the NMDOH action plan, expected in 2026.
HB 26: Nutritional Counseling and Medically Tailored Meals
Additional evidence is expected from HB 26 reporting, which requires HHSC to provide an annual report detailing:
- The number of nutritional counseling services delivered.
- The respective costs for Medicaid beneficiaries.
For pregnant women participating in the medically tailored meals pilot program, HHSC must collect data on:
- The rate of patient compliance with the medically tailored meal plan or other nutritional support services.
- Impact on the mother’s chronic health conditions.
- Maternal and infant health outcomes.
A comprehensive summary is due at the program’s conclusion in 2031. It is unclear whether interim outcomes will be released, although doing so could support quality improvement during program implementation.
HHSC Sunset Review
The 2026–27 Sunset Review represents a significant opportunity to evaluate HHSC’s capacity to implement NMDOH policies, integrate data systems, and strengthen oversight of managed care innovation in addressing members' non-medical needs. Under the Sunset Law, reviews can result in abolishing HHSC, restructuring the agency, or reassignment of functions to other state entities.
The last sunset review of HHSC, which occurred in 2014–15, recommended a series of management actions without statutory change, including:
- Evaluating Medicaid data trends.
- Coordinating managed care audit activities.
- Adding managed care representation to the Medical Care Advisory Committee.
Since then, HHSC has made significant strides in coordinating with managed care organizations to implement non-medical screening and data collection, as reflected in the initial HB 1575 report. For the upcoming sunset review, possible areas of focus include:
- Improving efficiency and accountability in Medicaid operations.
- Reducing fragmentation in oversight and redundancy across programs.
- Breaking down siloed procurement and data processes through further administrative consolidation.
Federal Policy Creates Uncertainty for Medicaid Coverage of NMDOH Services
Medicaid has been a key national driver in advancing state efforts to integrate NMDOH services into the health care delivery system. The two previous administrations expanded federal guidance and funding flexibilities to support these services within Medicaid. In response, states have increasingly implemented these options within their programs. However, signals from the current federal administration regarding NMDOH prioritization in Medicaid have been mixed, which could impact states’ integration efforts.
Guidance Rescissions — The CMS rescinded guidance from 2023 and 2024 detailing states’ options for NMDOH coverage in Medicaid. While this specific guidance was withdrawn, a broader guidance issued in 2021 remains active. State plans with previously approved NMDOH coverage are allowed to continue their programs, but future state applications to cover NMDOH services will now be reviewed on a case-by-case basis. While Texas’ Section 1115 demonstration waiver is approved through 2030, these changes could impact any new Texas proposals for Medicaid ILOS, 1915 waivers, and health services initiatives within the Children’s Health Insurance Program.
Federal Budget Cuts — The One Big Beautiful Bill Act (HR 1) makes major reductions in the federal contribution to the Medicaid program. For Texas, this could mean an estimated $31 billion cut to the federal match over the next 10 years. While HR 1 does not specifically exclude NMDOH services, the overall reduction in federal support may compel states to scale back benefits, narrow eligibility, reduce payment rates, or fund NMDOH services through alternative state-based payment mechanisms. Data collection from state legislation, like HB 1575 and HB 26, on program impact should also consider cost savings. This information could help shape future state funding decisions on NMDOH services, particularly given the changes to federal budgets.
Make America Healthy Again (MAHA) — The MAHA program promotes a prevention-focused approach that goes beyond medical services alone. By emphasizing the role of living conditions in shaping health outcomes, MAHA aligns with efforts to address health-related, non-medical needs. Integration of MAHA priorities in Medicaid and Medicare operations presents a significant opportunity for improving health outcomes. The MAHA Commission’s report highlights priority areas such as poor diet, lack of physical inactivity, social isolation, and environmental exposures. These non-medical factors can be effectively mitigated through evidence-based interventions, including medically tailored meals, exercise referral programs, nutrition and physical activity coaching, resource navigation, peer support, and home remediation services. Leveraging proven NMDOH strategies offers a pathway to strengthen the health care system’s focus on prevention and achieve meaningful improvements in population health.
Conclusion: Building Momentum for NMDOH Policy in Texas
The 89th Legislative Session reaffirmed Texas’ commitment to policy solutions addressing non-medical drivers of health and achieved important progress through Medicaid coverage options and maternal health supports. While these advances are significant, they remain narrowly focused, leaving opportunities to scale NMDOH interventions for other priority populations and health conditions.
The upcoming biennium will be pivotal. Key data from HB 1575 and HB 26 will inform data-driven policymaking, and the next sunset review offers an opportunity to strengthen HHSC’s innovation, integration, and oversight capacity. By leveraging these insights and building on legislative momentum, Texas can position itself as a national leader in integrating NMDOH strategies to improve health outcomes and contain health care costs.
This publication was produced on behalf of Rice University’s Baker Institute for Public Policy. Wherever feasible, the material was reviewed by external experts prior to its release. Any errors are the responsibility of the author(s) alone.
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author(s) and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s) and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.


