
Executive Summary
The Rural Health Transformation Program (RHTP) is a $50 billion Medicaid initiative to strengthen rural healthcare delivery through state-led transformation strategies. Although not required, most states’ applications included plans for addressing non-medical drivers of health, referred to by U.S. Centers for Medicare and Medicaid Services (CMS) as “health-related social needs” (HRSN). HRSN are the social and economic needs that “put individuals at risk for worse health outcomes and increased healthcare use.”
The RHTP application process offered states broad flexibility in outlining their plans to strengthen rural communities “by improving healthcare access, quality, and outcomes by transforming the healthcare delivery ecosystem.” States were not required to include HRSN services and faced competing priorities within the application constraints.
The prevalence of HRSN priorities across state applications reflects a widely held understanding of the importance of considering health-impacting non-medical needs when intervening to improve outcomes and controlling healthcare costs.
This analysis comes as states complete negotiations with CMS to revise their applications to fit within the awarded budget and make procurement decisions about how best to deploy this federal investment amid broader Medicaid financing pressures. The decisions made this year will determine whether HRSN services continue to be prioritized.
Moreover, the inclusion of HRSN strategies within the RHTP for states across the political spectrum may also reveal continued momentum and opportunities to build HRSN into other health system reform efforts. Many of the ideas proposed are not only suitable for rural healthcare but also for Medicaid beneficiaries more broadly.
State Approaches to Social Needs in Applications
The RHTP was passed as part of Section 71401 of Public Law 119‑2 (the One Big Beautiful Bill Act, OBBBA), which appropriates $10 billion annually from 2026 through 2030. It allowed states to compete for these funds to reimagine rural care delivery and improve health outcomes.
This program, administered by the new Office of Rural Health Transformation, focuses on five strategies to improve population health in rural communities:
- Make rural America healthy again by promoting preventive health and addressing root causes of disease.
- Sustainable access by improving the efficiency and sustainability of rural healthcare facilities.
- Workforce development through recruitment and retention strengthening activities.
- Innovative care focused on cost containment and improved quality.
- Technology innovation to promote efficient, secure, and accessible care.
The funding announcement further defined these priorities to provide examples of acceptable uses of funds, such as “promoting evidence-based, measurable interventions to improve prevention and chronic disease management.” States were required to include at least three of those strategies.
The application review process incentivized states to align their proposals with the law’s priorities. Through a competitive review process, CMS evaluated applications based on the following criteria:
- Financial sustainability.
- Measurable impact goals.
- Alignment with CMS reform efforts.
- Data reporting.
- Evaluation plans.
Half of the award amount was allocated as workload funding based on the proposal’s alignment with program goals and rural healthcare needs, while the other 50% was distributed evenly to approved states as baseline funding. Funding for subsequent years is contingent on achieving performance-based milestones, and states that do not meet these targets risk losing funding that may be redistributed to higher-performing states.
Because HRSN services were not a program requirement, their inclusion reflects an intentional strategy by states for improving prevention and chronic disease management. The most explicit connection to HRSN in the merit review is reflected in one of the technical score methodologies, which awards up to 100 points (out of a total of 1,500 technical points) for the quality of the proposal’s description of coordination between healthcare providers and community-based organizations for social services and preventive care.
On December 29, 2025, CMS announced that all 50 states applied for and received an RHTP award. Total award amounts vary across states, and funding per resident varies considerably. Analysis by KFF revealed that initial awards beginning in fiscal year 2026 averaged approximately $200 million per state; ranging from roughly $147 million in New Jersey to more than $281 million in Texas. On a per capita basis, this translated to less than $100 per rural resident in 10 states to more than $500 per rural resident in eight states. Texas, with the largest rural population in the United States and the largest monetary award in the first year, will receive the smallest payment per rural resident ($66).
Gaps in Existing Analysis of Social Needs Policy
Health outcomes are shaped by more than medical care alone. While access to quality healthcare is vital, it accounts for only 10%–20% of overall health outcomes. Instead, the health of a population is largely determined by social and economic factors, health behaviors, and the physical environment rather than clinical care. As policymakers seek to improve chronic disease outcomes, reduce preventable medical care, and contain costs, there is a growing interest in using Medicaid coverage to address these root causes of disease.
The RHTP provides a major new opportunity for states to test HRSN services at scale. Given the significant investment in the RHTP, multiple analyses have examined state applications, including:
- Allocation of state funds — KFF.
- Technology infrastructure — KFF.
- Potential for transformation of rural care delivery — The Commonwealth Fund.
- Funding levels relative to rural health needs — Penn LDI.
- Individual strategies, such as Community Health Workers — National Academy for State Health Policy (NASHP).
- Specific eligibility groups such as pregnancy/postpartum beneficiaries — NASHP.
However, little attention has been given to how states are using the RHTP to finance HRSN services within rural health transformation. This brief is the first known analysis of how states proposed incorporating HRSN services in their RHTP applications. By examining each state’s proposal, the analysis provides an early look at the various approaches that states are contemplating to integrate HRSN services into rural care delivery and financing.
Methodology
This brief summarizes how states included explicit coverage for HRSN services, typically described in the “Proposed Initiatives and Use of Funds” section of their RHTP applications. Each state’s application was reviewed via a full narrative read-through plus a targeted keyword search to identify proposed HRSN services.
For this analysis, services were included only if the state application clearly described direct coverage or infrastructure development for specific services — such as medically tailored meals or transportation — for individuals who qualify based on a health condition and an identified HRSN. Investments in general population health or community health without defined eligibility or service pathways were not classified as HRSN services for the purpose of this analysis. More detail about the review process is described in the Appendix.
This analysis focused on the narrative submitted to CMS in the original application and does not reflect actual implementation activities, as states are currently in the process of procuring services. Actual activities may differ as states ensure compliance with regulatory requirements and right-size their activities to their awarded amounts.
Common Strategies for Addressing Social Needs Across States
Within the broad parameters of the RHTP application, 45 states described HRSN services and supports in their application. For a summary of types and distribution of HRSN coverage options, see Table 1.
Table 1 — Health-Related Social Need Service Options by State
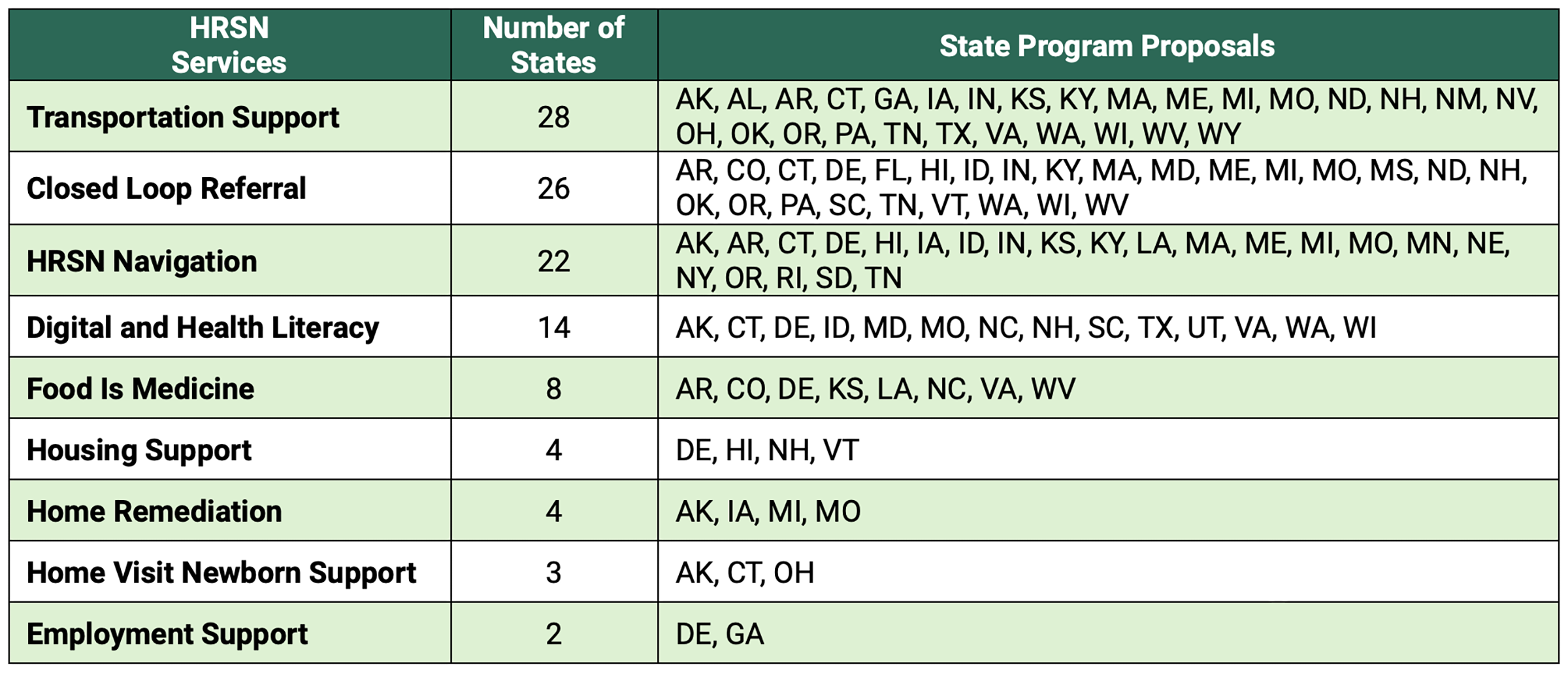
Non-emergency transportation support identified in 28 state applications, was the most common HRSN service. Medicaid already covers non-emergency medical transportation to doctors’ appointments, dentist visits, and pharmacies. However, RHTP applications proposed expanding the list of eligible destinations to include those offering non-medical services addressing HRSN. For example, the Rural Texas Strong application proposed non-emergent transportation that includes travel to “grocery stores that sell U.S. grown produce, dairy, and meat.”
Closed-loop referral systems were another common HRSN strategy, appearing in 26 state applications. These models generally proposed technology and coordination mechanisms to connect rural patients with community-based HRSN services and to verify HRSN service delivery. For example, Hawaii’s application proposed launching a new closed-loop referral system linking rural patients to HRSN services for health management and illness prevention. Their proposal also included infrastructure funding for technology and onboarding support for both healthcare and social service providers to ensure referrals result in service delivery.
HRSN navigation services were another leading strategy, which commonly identified community health workers as providers. For instance, the Kansas proposal included community health workers as providers of telehealth navigation for food is medicine and substance use care.
Digital and health literacy initiatives were built into the plans of several states, which is unsurprising given that technological innovation was a core goal of the RHTP. Utah’s proposal covered onsite and virtual training and technical assistance to implement, manage, and sustain digital literacy education. Their target audiences included patients, providers, and community members.
Food is medicine services were a strategy that often specified a particular targeted disease or health condition. Virginia’s proposal focused on participants with diabetes, incorporating technical assistance, data system integration, and coordination with community-based organizations to deliver food is medicine services and included evaluation of changes in average HbA1c levels.
Housing support was a strategy for individuals who met specific eligibility criteria based on a health diagnosis. Delaware proposed covering temporary housing, paired with integrated community services, for individuals with serious mental illness and substance use disorder.
Home remediation strategies were proposed for addressing underlying sources of health risk. Michigan proposed funding the repair and rehabilitation of single-family homes to mitigate asthma triggers and address safety hazards contributing to chronic disease.
Newborn and perinatal home visits were proposed by three states. Alaska’s plan proposed home visits to support maternal health, including lactation support, safe-sleeping practices, and postpartum depression screening.
Employment support was surprisingly rare, given the requirement for employment verification in the broader Medicaid program under the OBBBA. Georgia’s plan proposed funding vocational training and life skills counseling for those with an acquired brain injury.
Why States Diverged in Addressing Social Needs
Five states did not include an explicit description of HRSN coverage: Arizona, California, Illinois, Montana, and New Jersey (Figure 1). While several of these plans described infrastructure that could indirectly benefit HRSN, their descriptions were either too vague or focused instead on population health approaches for the general community, regardless of health diagnosis or risk.
Figure 1 — States Describing Health-Related Social Needs Coverage in Their Rural Health Transformation Program Application
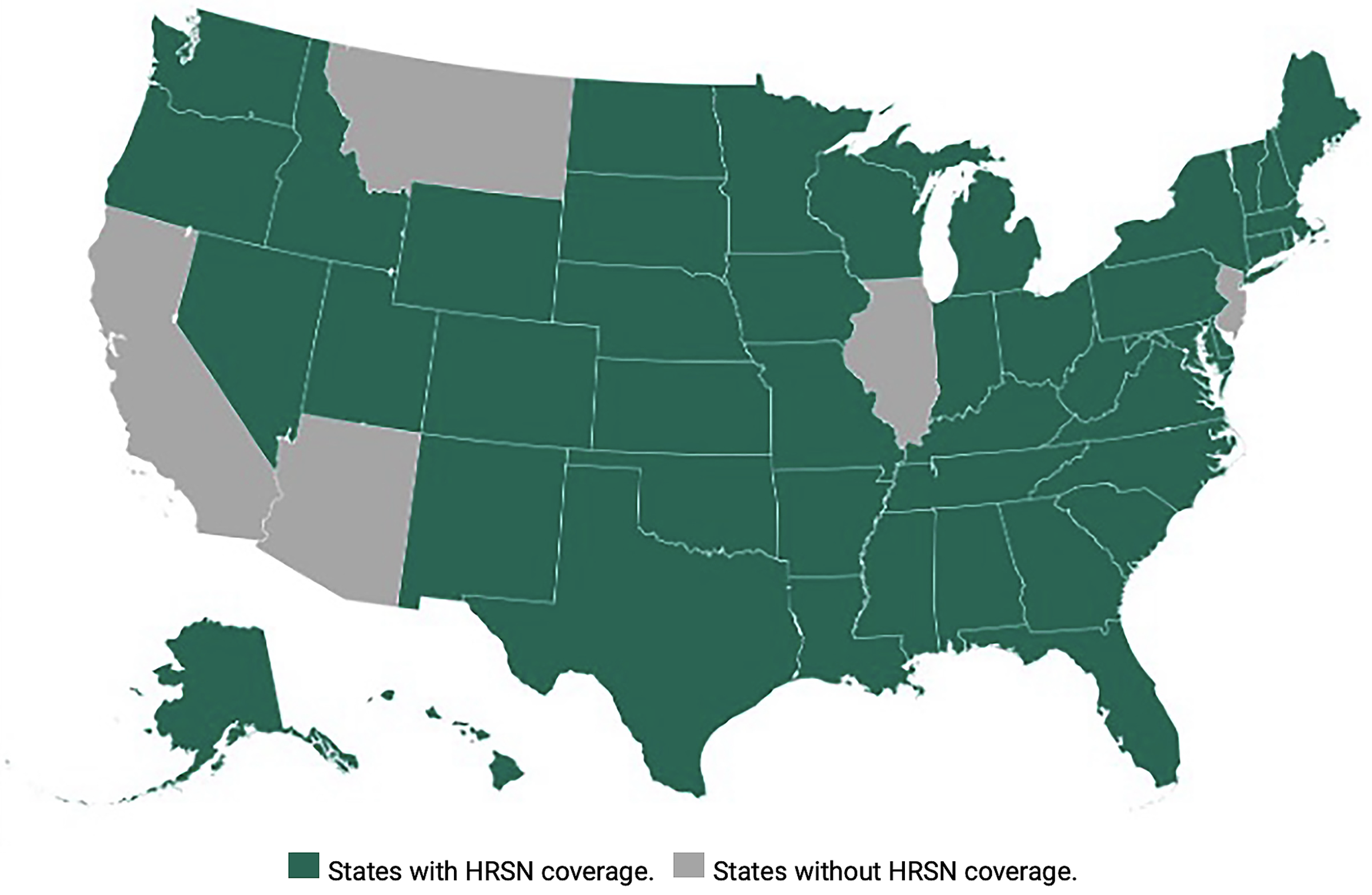
Notably, some states that have been leaders on HRSN coverage through their Medicaid Section 1115 demonstrations did not include these services in their RHTP applications. “Demonstrations” in the health policy context refer to experimental or pilot projects. This absence may reflect strategic decisions to use RHTP funds to fill gaps in more upstream public health investments not already financed through existing Medicaid authorities. For example, California’s plan includes community-based roles such as community health workers, midwives, and doulas focused on frontline (clinical) care, but does not describe their connection to HRSN community supports.
The Illinois proposal focused on public health priorities to prevent and manage disease. State officials indicated that, because Illinois was already covering HRSN services in its Section 1115 demonstration, the RHTP presented an opportunity to focus on stabilizing the broader rural healthcare system. Additionally, their focus on coverage of medical services reflected their interpretation of the RHTP goals as outlined in the OBBBA and the notice of funding opportunity.
Arizona did not explicitly describe HRSN services in its application, but state officials indicated that this reflected a deliberate decision to maintain flexibility in how RHTP funds would be awarded rather than a decision to exclude HRSN services. Arizona’s application ties funding to eligible activities aligned with RHTP goals rather than specific programs. As a result, initiatives addressing HRSN may ultimately be funded if they demonstrate a direct connection to program objectives and comply with CMS requirements.
States’ choices about inclusion of HRSN coverage reflect distinct strategies: targeted, patient-level services versus broader population health investments.
Policy Implications and Recommendations
The RHTP’s structure means that performance-based funds are not guaranteed year to year. Because states will be evaluated annually to determine funding renewals, HRSN strategies will face immediate accountability for delivering measurable improvements in rural healthcare delivery.
As implementation begins in 2026, it will be important to monitor the extent to which states’ original HRSN service plans translate into practice and ultimately whether these investments improve the performance of rural healthcare. For policymakers, the next phase of the RHTP will test whether integrating HRSN services into care delivery produces measurable returns under real-world performance rating constraints.
The following list describes key recommendations for policymakers, Medicaid agencies, managed care organizations, and rural health systems as implementation moves forward:
- Prioritize evaluation and standardized outcome measurement for HRSN services. While most states proposed HRSN services, fewer defined evaluation metrics tied to utilization, health outcomes, or costs. CMS and states should prioritize standardized measures for HRSN interventions to determine which models improve outcomes and/or reduce avoidable utilization in rural settings.
- Strengthen infrastructure for cross-sector coordination and closed-loop referral. The prevalence of applications seeking funding to support navigation and closed-loop referral systems demonstrates that states increasingly view coordination between healthcare and community-based organizations as foundational rather than a supplemental activity. Future implementation efforts should focus on interoperability, referral verification, data-sharing standards, and sustainable financing mechanisms that allow community-based organizations to participate in Medicaid-supported healthcare delivery. Existing federal and state investments in electronic health information exchanges can help integrate HRSN-related data into shared systems, creating a more complete picture of services across clinical and community settings.
- Use the RHTP to identify sustainable operational models. Previous large-scale Medicaid transformation efforts, such as the Delivery System Reform Incentive Payment (DSRIP) program, demonstrated that implementation infrastructure can wither once demonstration funding ends. States should use the RHTP implementation period to identify which HRSN strategies deliver measurable value and to develop long-term financing pathways that sustain successful programs, workforce models, and community partnerships beyond this initial RHTP investment.
- Integrate HRSN services into durable Medicaid financing models. Policymakers should consider how HRSN strategies can be integrated into longer-term Medicaid financing pathways, including managed care contracting, value-based payment arrangements, and other sustaining reimbursement mechanisms beyond the five-year RHTP funding period.
Conclusion
Established through the OBBBA, the RHTP was designed to drive large-scale transformation of rural healthcare delivery. The analysis revealed that while HRSN services were included in the large majority of state RHTP proposals, the types of services and their prevalence across states varied substantially. However, the widespread adoption — and the willingness to try different approaches across politically and geographically diverse states — signals a growing confidence in these models, despite the financial pressures facing rural healthcare. States are no longer treating HRSN coverage as pilot-stage innovations, but as core components of care delivery and long-term cost-containment.
This prioritization is noteworthy in light of the broader Medicaid financing challenges states are facing. Between 2025 and 2034, federal Medicaid funding to states is projected to drop by an estimated $664 billion due to changes in provisions such as work requirements, eligibility redetermination frequency, state-directed payments, and provider taxes. The $50 billion RHTP investment will do little to offset this loss. Against this backdrop, the decision by many states to dedicate scarce RHTP dollars to HRSN services, rather than exclusively to medical care, is significant.
The broader policy challenge is whether these successful HRSN strategies can survive beyond federally funded programs. As states move into RHTP implementation, the true test will be whether HRSN services become a sustained element of rural healthcare delivery or remain a temporary, demonstration-era expense.
Appendix
Review Method
Analysis was conducted via a complete read-through of the narrative and manual searches of predefined key terms (e.g., food, transportation, digital literacy, etc.). An independent review of all 50 states’ applications was conducted by authors Charles W. Mathias and Carlos A. Cruz, and an additional validation review on a subset of state applications was conducted by author Kathryn Jantz. Where the application language was unclear, the authors sought clarification from state officials through email correspondence conducted in May and June of 2026. Responses were received from Illinois and Arizona.
Materials
A full list of the individual RHTP applications and program abstracts was retrieved from the Rural Health Information Hub.
Inclusion/Exclusion
For this analysis, services were included only if the state application clearly described direct coverage or infrastructure development for specific services — such as medically tailored meals or transportation — for individuals who qualify based on a health condition and an identified HRSN need. Broader investments in population health or community health without defined eligibility or service pathways were not classified as HRSN services and thus not included. This approach is consistent with CMS differentiation between HRSN and social drivers of health criteria.
Proposals that referenced broader system improvements or population health strategies but did not clearly delineate individual-level HRSN services were excluded. Excluded initiatives included investments in community health workers and health information exchange infrastructure that did not specify how they would be applied as a service to address an individual’s HRSN. While each of these strategies can play an important enabling role in addressing HRSN, the available application materials did not provide sufficient details to confirm that they were structured as direct benefits targeting specific HRSN.
Three services that were particularly nuanced in whether they met the definition of addressing an HRSN were transportation, food, and housing.
- Transportation services to medical appointments or non-medical services (e.g., grocery stores) were included so long as they were linked to a patient care plan and a patient’s health barrier. Medical treatment in place was excluded as an HRSN. Inclusion of both medical and non-medical transport has been used in health-related social needs screening definitions. Transportation to medical or non-medical services has been described as crucial for chronic disease management.
- Food is medicine coverage was included if the application defined beneficiary services, where the composition of the food support was linked to a health condition at an individual patient level. Provider education on food is medicine without a defined service pathway was excluded. Services, such as broader, lighter-touch strategies for food insecurity, such as strengthening networks of local food sources, without a tailored diet, were excluded. This distinction reflects an ongoing debate within the field: some conceptualize food is medicine and food insecurity interventions as part of the same continuum, while others treat them as complementary but adjacent interventions in terms of how they are delivered, targeted, and financed.
- Housing support was included if the housing service was for patients. Many proposals included workforce housing, but these were excluded in the HRSN service coding.
This publication was produced by Rice University’s Baker Institute for Public Policy. Wherever feasible, the material was reviewed by outside experts prior to release. Any errors or omissions are solely the responsibility of the author(s).
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author(s) and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s) and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.


