
Executive Summary
Food and its impact on health have come to the forefront of policy attention. During the 89th Texas Legislative Session in 2025, several bills were introduced proposing Medicaid coverage for food interventions designed to address specific medical diagnoses. These proposals demonstrate growing interest in using food as a clinical tool, distinct from general nutritional assistance.
Policies addressing food and health cut across the major programs, including Medicaid, the Supplemental Nutrition Assistance Program (SNAP), and the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC). Recognizing the distinctions in purpose, eligibility, funding mechanisms, and allowable foods across these programs is essential for designing policies that achieve defined health goals.
This report examines each program and recommends targeted use of Medicaid for high-cost diet-related conditions and encourages full participation in SNAP and WIC to prevent disease progression and reduce long-term spending.
Programs for Nutrition and Health
Pressures from both federal policy priorities and state budget constraints are driving broader policy conversations about whether food interventions should be covered as part of health care. During the 89th Texas Legislative Session, lawmakers introduced bills to authorize Medicaid funding for food interventions. Three bills proposed using Medicaid managed care funding via an In Lieu of Service (ILOS) mechanism to cover food interventions like medically tailored meals for specific medical conditions.
ILOS is a Medicaid managed care funding mechanism that states may use to authorize coverage for services that are medically appropriate, cost-effective, and may reduce the need for future medical services. HB 26 was passed into law; it covers nutritional counseling for Medicaid beneficiaries broadly and a pilot program for medically tailored meals for pregnancies that are high-risk due to gestational diabetes, hypertension, and obesity.
While these ILOS bills demonstrated legislative interest in Medicaid funding of food interventions to improve health, they also raise questions about the distinctions between federal health and food programs and the states’ authority to flexibly apply them to solve specific goals. Although Medicaid, SNAP, and WIC share similarities, their purposes, scopes, and delivery mechanisms differ significantly. This report provides a breakdown of the policy distinctions between these food and health programs.
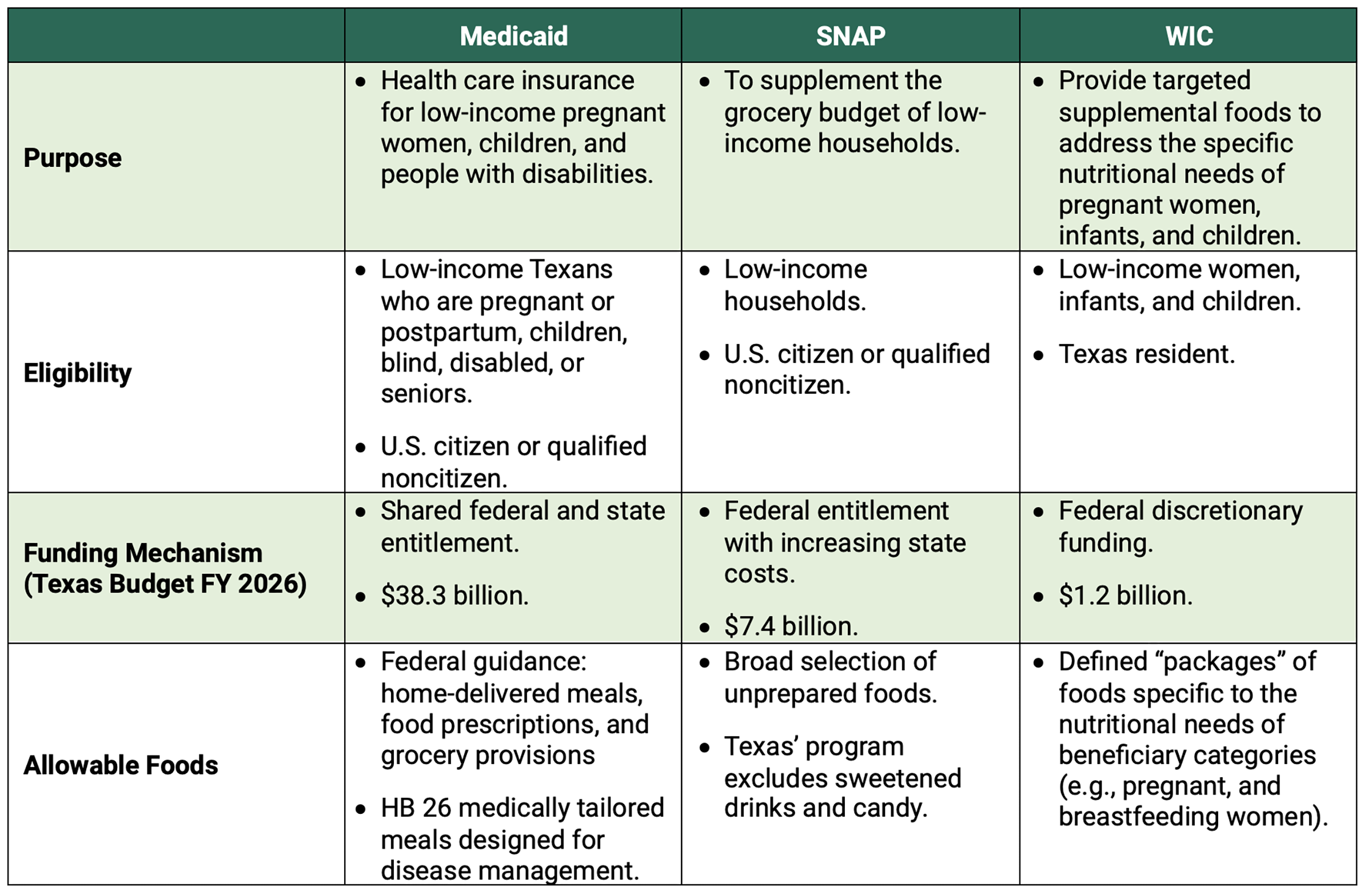
Table 1 summarizes key distinctions across programs, including the programs’ purpose, eligibility criteria, funding structure, and allowable food benefits.
Table 1 — Medicaid, SNAP, and WIC: Purpose, Eligibility, Funding, and Food Benefits
Statutory Roles of the Medicaid, SNAP, and WIC Programs
The congressional intent underlying Medicaid, SNAP, and WIC reflects distinct and complementary federal approaches to health and nutrition for low-income beneficiaries.
Medicaid
Medicaid is a public health insurance program that provides coverage for low-income pregnant women, children, and individuals with disabilities. As described by the Centers for Medicare and Medicaid Services (CMS), “Medicaid provides health coverage to low-income people and is one of the largest payers for health care in the United States.”
Congressional Intent
Medicaid was established in 1965 under Section 1901 of the Social Security Act amendments:
“For the purpose of enabling each State, to furnish (1) medical assistance on behalf of families with dependent children and aged, blind, or permanently and totally disabled individuals, whose income and resources are insufficient to meet the costs of necessary medical services, and (2) rehabilitation and other services to help such families and individuals attain or retain capability for independence or self-care, there is hereby authorized to be appropriated for each fiscal year a sum sufficient to carry out the purposes of this title.”
This statutory language reflects Medicaid’s primary role as a public health insurance program, with services defined as health-related.
SNAP
SNAP is the largest federal program funding food for low-income families. The U.S. Department of Agriculture (USDA) describes SNAP as providing “food benefits to low-income families to supplement their grocery budget so they can afford the nutritious food essential to health and well-being.”
Administered through the USDA, the SNAP program reflects federal efforts to address hunger through agriculture, poverty, and public health policies. SNAP is one of the USDA’s Nutritional Assistance Programs, whose collective purpose is to “increase food security and reduce hunger in partnership with cooperating organizations by providing children and people with low income access to food, a healthy diet, and nutrition education in a manner that supports American agriculture and inspires public confidence.”
Congressional Intent
In the Food Stamp Act of 1964, which founded the program, Congress declared that its purpose is “to promote the general welfare, that the Nation’s abundance of food should be utilized cooperatively by the States, the Federal Government, and local government units to the maximum extent practicable to safeguard the health and well-being of the National population and raise levels of nutrition among low-income households.” SNAP’s statutory language emphasizes food access, rather than health care.
WIC
WIC is a more specific federal food program focused on the unique nutritional needs of women, infants, and children. Like SNAP, WIC is administered by the USDA as one of the Nutritional Assistance Programs. The USDA describes the purpose of WIC to “safeguard the health of low-income pregnant, postpartum, and breastfeeding women, infants, and children up to age 5 who are at nutritional risk by providing nutritious foods to supplement diets, information on healthy eating, breastfeeding promotion and support, and referrals to health care.”
Congressional Intent
The WIC program was established in 1975 as a permanent program under the “Special Supplemental Food Program” of P.L. 94–105, the National School Lunch Act and Child Nutrition Act of 1966 Amendments of 1975. The program was created to “provide supplemental nutritious food as an adjunct to good health care during such critical times of growth and development in order to prevent the occurrence of health problems.” This framing reflects WIC’s role as a nutrition-specific intervention, closely linked to, but distinct from, medical care.
Eligibility Requirements for Each Program
Medicaid Eligibility
Medicaid provides health insurance coverage for eligible low-income Texans. Eligibility focuses on pregnant women and children, the blind or otherwise disabled, and seniors with low incomes. These are the monthly income and eligibility thresholds:
- Pregnant and postpartum women (up to 12 months): $2,583 or less for a single-person household, plus approximately $907 for each additional household member.
- Children: $2,635 or less per month, plus $926 for each household member.
- Elderly and people with disabilities: Income up to 300% of the federal poverty level.
To qualify for Medicaid, individuals must be Texas residents and U.S. citizens, nationals, or qualified noncitizens, such as:
- Lawful permanent residents.
- Individuals granted asylum, refugee status, or withholding of deportation.
- Individuals lawfully residing under the Compact of Free Association.
- Noncitizens who have held a qualified immigration status for at least five years.
SNAP Eligibility
SNAP program beneficiaries are people living in low-income households. Eligibility criteria include monthly income limits and work requirements for some adults. Monthly income limits are $2,152 for a single person and $757 more per additional household member. Work requirements apply to able-bodied adults without dependents, except for certain exclusions, including pregnancy.
Following the passage of the Reconciliation Act of 2025, SNAP benefits are restricted to citizens or nationals of the U.S. or certain qualified noncitizens — lawfully admitted permanent residents, those granted asylum or refugee status, persons lawfully residing under the Compact of Free Association; certain American Indians born abroad; and certain Hmong or Laotian Vietnam era tribal members.
WIC Eligibility
Similar to SNAP, the WIC program benefits low-income populations, but eligibility is restricted to women, infants, and children under 5 years old. Women are eligible if they are pregnant, up to six months postpartum, or up to one year postpartum if breastfeeding.
Income Eligibility Requirements
One of these criteria must be met:
- Program participation: Covered by Texas Temporary Assistance for Needy Families (TANF) or SNAP.
- Income threshold: Household income below 186% of the federal poverty level.
In 2025, the Texas monthly income limits were $2,413 for a single person and $848 per additional household member.
Nutritional Risk Requirements
In addition to income criteria, states are also required to assess nutritional risk of beneficiaries. In Texas, WIC screens for two categories of nutritional risk:
- Medically-based risks such as a history of poor pregnancy outcome, underweight status, or iron-deficiency anemia.
- Diet-based risks, such as poor eating habits, that can lead to poor nutritional and health status.
WIC participants must live in Texas. Citizenship or immigration status is not considered for eligibility determination.
Texas Implementation of Program Enrollment
Medicaid, SNAP, and WIC have distinct eligibility thresholds, although their shared focus on low-income populations means many beneficiaries qualify for more than one program. In debates over Medicaid coverage of food, co-enrollment in SNAP was cited as an alternative source of funding for food. The argument was that Medicaid coverage of nutritional education could enable beneficiaries to make healthy food choices using their SNAP or WIC benefits.
In practice, however, there are significant gaps in co-enrollment across Medicaid, SNAP, and WIC. A 2023 USDA report found that nationalwide only 42% of women in SNAP and 64% of women in Medicaid were enrolled in WIC. No publicly available database tracks individual co-enrollment across the three programs. The USDA report also finds that existing state-level co-enrollment data are too unreliable to inform policymaking.
Texas has sought to streamline co-enrollment through integrated application and eligibility systems and outreach efforts. However, these systems have faced technical challenges that delay paperwork processing, resulting in a significant backlog in enrollment. In the 89th Session, Texas authorized $300 million to modernize the Texas Integrated Eligibility Redesign System (TIERS) and hire additional staff through 2030 to improve efficiency in benefit application processing.
Funding and Cost Structures
Federal food and health coverage programs are funded either as entitlements or through discretionary appropriations. Entitlement programs — including Medicaid and SNAP — must cover eligible beneficiaries and are not limited by annual appropriations. In contrast, discretionary programs such as WIC are funded through the annual appropriation process, with total federal spending capped at the appropriated amount.
Medicaid is a federal entitlement program. Costs are shared between states and the federal government. The sharing rates are defined by the Federal Medical Assistance Percentage (FMAP), which varies by state. The 2026 FMAP for Texas is 59.83% (the federal coverage), with the state responsible for the remaining 40.17% of Medicaid costs. For fiscal year 2026, Texas budgeted $37.5 billion in SB 1 for Medicaid client services, plus $793 million for administrative costs.
SNAP is a federal entitlement program. Under longstanding policy, federal funds covered 100% of SNAP benefits for households, while administrative costs were split evenly between federal and state funding. Following the Reconciliation Act of 2025, states now face a greater share of administrative costs (75%), an increased administrative burden due to work-verification requirements, and liability for up to 15% food benefit costs if the payment error rate exceeds federal thresholds. Prior to these changes, the fiscal year (FY) 2026 estimated federal budget for SNAP household benefits for Texas was approximately $7.2 billion, and Texas’s share of administrative costs is budgeted at $244 million. Despite being an entitlement, the distribution of SNAP benefits was interrupted in 2025 during the federal government shutdown over the budget bill.
WIC is a discretionary federal grant program. It is funded through annual appropriations by Congress, and the amount may change each year based on current priorities. Federal funds are distributed to states primarily through grants from the USDA Food and Nutrition Service. Unlike SNAP, states are not required to cover the WIC program’s administrative costs. In Texas, WIC funds are treated as rebate revenue and support the approximately $1.2 billion allocated for WIC client services for FY 26, serving 796,000 beneficiaries.
Food Benefits and Program Design
During the 89th Session, lawmakers debated using Medicaid coverage of food as an intervention to address specific health conditions rather than nutrition assistance generally. The effectiveness of food-based health interventions depends on tailoring meals to the specific health conditions they are intended to address. In this approach, food functions similarly to medication: it is prescribed in a particular formulation (nutritional content, dosage, and duration) to achieve a targeted health outcome.
HB 26 Pilot Project for Targeted Pregnancy Nutrition Benefits
As a public health insurance program, Medicaid’s coverage of food has focused on targeted nutritional supports tied to specific health conditions and clinical outcomes. The HB 26 pilot project targets pregnancy with a diet-related health condition — including gestational diabetes, hypertension, and obesity — that may contribute to a high-risk pregnancy or birth complications.
The pilot covers medically tailored meals paired with nutritional counseling. The law defines a medically tailored meal as “a meal designed by a registered dietician as part of a treatment plan to improve an individual ’s health outcomes and chronic disease management,” ensuring an alignment between the selection of foods and the targeted clinical condition. These diagnoses require a specific dietary plan that differs from the standard WIC food packages, which are designed to address other pregnancy-related nutrition risks such as anemia or low maternal weight.
When using food as an intervention for a diagnosed health condition, selecting which foods to eat and avoid is essential. The following sections summarize the coverage of allowable foods within Medicaid, SNAP, and WIC.
Medicaid Covered Foods
As a public health insurance program, Medicaid covers food primarily through three policy mechanisms:
- Section 1115 demonstration waivers: Budget-neutral pilot programs that allow states to test innovative coverage and delivery models.
- Section 1915 waivers: Home and community-based services designed to keep beneficiaries with long-term care needs out of institutional care.
- In lieu of services (ILOS): Managed care organizations’ option to substitute cost-effective services, including food interventions, in place of traditional medical treatment.
Guidance from CMS — November 2023 and December 2024 — provides examples of allowable food benefits within the Medicaid program. This guidance identified three specific categories of food coverage: home-delivered meals, food prescriptions, and grocery provisions.
- Home-delivered meals: Provide prepared meals to beneficiaries who meet state-defined health eligibility criteria. Examples include “Medically tailored meals to individuals with nutrition-sensitive conditions (e.g., pregnant individuals, individuals with diabetes).” Some states, such as North Carolina, offer both medically tailored meals — designed by a dietitian to address a specific health condition — and general healthy meals that follow dietary guidelines. States typically reassess beneficiaries’ meal plans and qualifying conditions on an ongoing basis; for instance, North Carolina’s Medicaid 1115 waiver requires a eligibility review every three months.
- Food prescriptions: Offer specific categories of foods, rather than defining particular meals. Examples include fruit and vegetable prescriptions, protein boxes, food pharmacies, and health food vouchers. The food categories are selected based on the nutritional needs of specific health conditions and evidence linking dietary change to improved health outcomes. Food prescriptions are commonly administered as vouchers redeemable for qualifying food items.
- Grocery provisions: Provide the widest latitude for food coverage. Also referred to as pantry restocking, grocery provisions typically focus on ensuring a sufficient quantity of food rather than specific food types. This coverage is specified for beneficiaries at high health risk and is intended to prevent unnecessary acute care admission or institutionalization.
Key Points: Medicaid Covered Food
Coverage of food under Medicaid varies by the type of intervention. Medically tailored, home-delivered meals have the most direct alignment between food and the dietary needs of a specific health condition. This approach is unique to Medicaid and distinct from SNAP or WIC.
Food prescriptions focus on defined categories of food and are similar to the WIC approach, which targets the specific nutritional needs of pregnant women. Grocery provisions within Medicaid are similar to SNAP, offering a broader range of foods to ensure sufficient total dietary intake.
Beyond defining what foods are allowed, Medicaid policies also limit how much (dosage) and how long (duration) coverage lasts. These limits depend on the funding mechanism the state uses:
Quantity (Dosage)
- 1115 waivers: Up to three meals per day.
- ILOS and 1915 waivers: Fewer than three meals per day.
Duration
- 1115 waivers: Limited to a maximum of six months.
In 2025, the 2023 and 2024 CMS guidelines were rescinded. As a result, these food coverages — though not explicitly precluded — will be evaluated on a case-by-case basis for new state plan applications. Previously approved waivers were not affected.
SNAP Covered Foods
Historical Context
Understanding the debate over allowable foods in SNAP requires a historical context of the program. From its origins as an agricultural intervention to today’s focus on nutritional support, SNAP has evolved in response to new policy goals. This evolution reveals how today’s debates are rooted in precedents, reflecting long-standing tensions between broad access, administrative demands, and dietary quality.
The current SNAP program is an evolution of the Depression-era Food Stamp Program of 1939, which was designed to use agricultural surpluses to relieve hunger among low-income households. Participants in the program contributed to the cost of food. For every dollar contributed, participants received $1 in orange stamps and 50 cents in blue stamps.
While orange stamps were redeemable for a wide range of food, blue stamps could only be used for designated surplus agricultural commodities — such as dairy, flour, and pork; surplus status was designated by the Secretary of Agriculture. This augmented food budgets by 50% and incentivized demand for certain foods, helping to stabilize agricultural prices. The initial iteration of the program was discontinued in 1943 because World War II changed the conditions of agricultural market surpluses.
The Food Stamp Program of 1961 was introduced as a pilot program during President John F. Kennedy’s administration. Again, it was a buy-in program in which participants received more stamps than they paid for. It eliminated the blue stamp tiering, meaning coverage no longer incentivized the purchase of agricultural surplus foods. As a result, the program covered a broad range of foods.
As part of President Lyndon B. Johnson’s War on Poverty, Congress passed the Food Stamp Act to make the program permanent in 1964. While the House version of the Food Stamp Act would have prohibited the use of food stamps to purchase soft drinks and luxury foods, those provisions were not enacted.
Since its inception, the SNAP program has undergone policy revision, changing the structure of food coverage. Key policy landmarks include:
- Set benefit amounts to the cost of a nutritionally adequate diet (1971).
- Removed the purchase requirement, allowing recipients to receive food stamps without an upfront buy-in (1977).
- Repeatedly adjusted monthly household benefit benchmarks to reflect changing economic conditions (1981,1982, 1988, 1990, 2008, 2009, 2021).
- Enhanced nutritional standards for covered foods (2010).
- Introduced incentives to purchase fruits and vegetables (2014).
- Revised the baseline benefit size and established new limits on future benefit increases (2025: the Reconciliation Act).
Present Day
Under current law, SNAP beneficiaries have a wide range of food options. SNAP benefits may be used to purchase most foods intended for home consumption, including fruits, vegetables, meats, dairy products, breads, cereals, snack foods, and seeds or plants for household food production. However, benefits may not be used for alcohol, tobacco, vitamins and supplements, controlled substances, live animals, hot prepared meals, or nonfood items.
Texas Gov. Greg Abbott has been critical of the program’s breadth of food options, stating, “SNAP was created to increase access to nutritious food; however, many SNAP purchases are for food with little to no nutritious value.” Texas received approval for a waiver to modify the food list to exclude sweetened drinks and candy for two years beginning on April 1, 2026. As part of the waiver, Texas will evaluate its impact on SNAP participants and retailers.
Thus far, 18 states have been approved for Food Restriction Waivers to exclude “non-nutritious items like soda and candy” from SNAP benefits. While most waivers focus on sugary drinks and candy, others go further.
- Arkansas: Excludes drinks that are less than 50% natural fruit or vegetable juice.
- Tennessee: Excludes processed foods and beverages.
- Louisiana: Excludes energy drinks.
- Iowa: Excludes fruit bars, caramel wraps, sweetened coconut, marshmallows, and candy-coated popcorn.
Originally designed to stabilize agricultural markets, SNAP has shifted its focus from basic hunger relief toward higher-quality nutritional goals. The current series of waivers reflects a period of active experimentation, as states evaluate whether restricting certain foods can improve diet quality or health without undermining food access. These changes demonstrate growing policy interest in SNAP as a nutrition-assistance program and as a mechanism supporting health.
WIC Covered Foods
Unlike Medicaid and SNAP, WIC was designed from its inception to align food benefits with the specific nutritional needs of pregnancy, infancy, and early childhood. Over time, federal statutes and USDA guidance have refined the selection of foods, known as “food packages,” to address the typical nutritional deficits of low-income beneficiaries. The WIC food benefit is designed to be supplemental, filling nutritional gaps, and is not intended as a complete diet for beneficiaries. Participation in WIC does not preclude enrollment in SNAP, and the two programs are designed to operate in parallel.
The WIC program was first established in 1975. While the statute did not specify individual foods, it stipulated that allowable foods must contain “high-quality protein, iron, calcium, and vitamins A and C.” The statute also authorized foods “commercially formulated” specifically for women or infants at the discretion of the Secretary of Agriculture. The law also allowed flexibility for “medical and nutritional objectives and cultural eating patterns” of beneficiaries.
Over time, WIC policy has periodically adjusted which foods qualify for coverage. These policies define allowable foods, including those foods containing nutrients determined by nutritional research to be lacking in the diets of pregnant, breastfeeding, and postpartum women (1978), adding more specific food packages (1980), making coverage revisions to align with changing dietary guidelines (2007 and 2024), and allowing food substitutions for participant preferences (2014).
Under current USDA guidance, WIC-eligible food packages specify maximum monthly allowances of nutrient-dense foods for beneficiaries. These allowances vary across the three distinct food packages for women, based on pregnancy status: pregnant, postpartum (up to six months), or breastfeeding (up to 12 months postpartum). Food packages for pregnant and postpartum women include milk, eggs, breakfast cereal, fruit and vegetables, juice, whole wheat bread, canned fish, legumes, and peanut butter.
By law, the USDA must review WIC food packages periodically and update them based on the latest nutritional science, federal dietary guidelines, and program implementation considerations. The following organizations have provided input on WIC food package definition, as noted below:
- The National Academies of Sciences, Engineering, and Medicine serves as an independent scientific advisor, providing evidence-based recommendations to the USDA. Their landmark reports include the “WIC Food Packages: A Time for Change” (2006) and “Review of WIC Food Packages: Improving Balance and Choice, Final Report” (2017).
- The U.S Department of Health and Human Services (HHS) coordinated with the USDA on “Dietary Guidelines for Americans” and “Dietary Reference Intakes,” which set nutritional benchmarks used by WIC to ensure food packages address nutritional gaps.
- The USDA Food and Nutrition Service influences WIC food packages by translating statutes, dietary guidance, and scientific recommendations into rulemaking that defines allowable foods, quantities, and implementation requirements.
Policy Recommendations
Texas has legislative and administrative influence over the delivery of health and nutritional supports through the Medicaid, SNAP, and WIC programs. Because the scope of that influence varies by program, Texas should use different strategies to leverage each program’s design to achieve health and cost goals.
Targeted Medicaid Priorities
The flexibility within Medicaid provides Texas with a direct policy mechanism to address priority health conditions. States can customize their Medicaid programs within federal standards and subject to federal approval; Texas has obtained such approval to cover additional services and populations. As demonstrated in HB 26, Medicaid’s ILOS authority allows Texas to target specific health populations and outcomes, define covered services and provider types, and do so on a cost-neutral basis. These flexibilities enable the state to cover customized interventions that improve health and potentially avert higher downstream health care costs.
Texas currently uses these policy tools to improve maternal and birth outcomes, yet they are also applicable to other diet-related conditions. To date, policymakers have taken a relatively narrow approach, limiting Medicaid’s food coverage to pregnant and postpartum women. Medicaid covered approximately 53% of Texas’ 388,114 births in 2022. A significant opportunity exists to improve health outcomes and constrain the state’s Medicaid spending by extending these policy solutions to other prevalent, high-cost conditions such as diabetes and kidney disease — both of which show strong clinical response to medically tailored meals.
Applying Medicaid Authority to Address High-Cost Conditions
Diabetes is one of the most costly and preventable diet-related health burdens in the Medicaid program. Over 630,560 adults in Texas Medicaid have a diabetes diagnosis, costing the program an estimated $6.2 to $8.1 billion in 2021 alone. In the 89th Session, the legislature passed a budget rider for a Diabetes Prevention Program, which directs HHSC to study the “cost-effectiveness and feasibility of implementing and administering a diabetes prevention program for Medicaid recipients, including alternative interventions for Medicaid recipients at risk of developing Type 2 diabetes.” Medically tailored meals and other dietary interventions are keys to diabetes prevention strategies. National estimates indicate that medically tailored meals for diabetes can avert 63,000 hospitalizations, resulting in net annual savings of $1.4 billion for Medicaid. The outcomes of the Texas Diabetes Prevention Program study are due Nov. 1, 2026, and may serve to inform legislation in the 90th legislative session.
Kidney disease is another prevalent, diet-responsive cost driver in Texas Medicaid. Kidney disease impacts more than 1 in 7 adults, which translates to about 3 million Texans. The Texas Kidney Health Care program, which provides medical and transportation support for the most severe, end-stage kidney disease, cost over $8.2 million in 2025, a 38% increase over 2024. Evidence from Texas shows that medically tailored meals can significantly delay the progression of kidney damage, potentially averting the development of kidney disease and associated medical costs. By leveraging the policy authorities and managed care arrangements established under HB 26, Texas can efficiently scale these interventions, improve health outcomes, and reduce long-term costs.
Full Participation in SNAP and WIC
While Medicaid offers a targeted approach, SNAP and WIC provide a broader population health opportunity. Texas ranks second-to-last in food security. Texas can influence SNAP and WIC participation through administrative choices and waivers that affect eligibility, enrollment, and verification. The state’s $300 million TIER modernization project aims to reduce coverage gaps and maximize enrollment efficiency across SNAP, WIC, and Medicaid. By addressing food insecurity — which is linked to the development of diabetes and end-stage kidney disease — improving SNAP and WIC coverage can prevent disease progression and reduce reliance on intensive medical care.
While Medicaid remains a much larger state budget expenditure, the 2025 Reconciliation Act substantially increases Texas’ share of SNAP costs. This fiscal shift will be an important issue in the 90th Legislative Session as lawmakers consider the unprecedented increase in state costs compared to budgets from previous sessions. Decisions about increased state funding of SNAP benefits will need to be evaluated in the context of the economic and health care consequences of these services.
Research from the USDA reports that for every $1 in SNAP spending, $1.54 in gross domestic product (GDP) is generated. This net benefit reflects multiplier effects across employment, food, health care, housing, transportation, and other goods and services. SNAP participation may also create notable spillover savings within Medicaid. Studies link SNAP enrollment to lower rates of hospitalization and emergency department use, reducing annual Medicaid expenditures.
While the 2025 Reconciliation Act may soon require Texas to fund up to 15% of SNAP benefit costs, the state already finances 40.17% of Medicaid costs in 2026. Because Texas bears a larger share of Medicaid expenses, any SNAP investment that reduces medical utilization — and Medicaid spending — may yield a considerably greater net fiscal benefit for the state.
Conclusion
The 89th Texas Legislative Session highlighted a growing interest in using food interventions to improve health outcomes among Medicaid beneficiaries. As policymakers explore funding options, it is essential to recognize the distinct roles of Medicaid, SNAP, and WIC. Each program has different statutory purposes, eligibility rules, funding mechanisms, and benefit structures. While they may supplement each other, they are not duplicative or interchangeable.
When food is used to treat a diagnosed health condition, Medicaid is uniquely positioned to serve as the payer through targeted, time-limited, and outcome-driven design. HB 26 demonstrates that Texas can thoughtfully leverage Medicaid policy tools to address priority health conditions while maintaining cost neutrality.
Capitalizing on the HB 26 pilot program, Texas has opportunities to apply medically tailored meals to other high-cost, diet-modifiable conditions, such as diabetes and kidney disease. Using Medicaid’s ILOS mechanism provides an efficient way to advance the state’s health goals while potentially reducing substantial health care costs. Improving participation in SNAP and WIC enrollment can further reduce downstream Medicaid spending by addressing food insecurity at the population level.
As state costs and administrative pressures grow across federal programs, aligning these policy mechanisms will be increasingly important. Strategic use of Medicaid’s flexibility, combined with robust participation in SNAP and WIC, offers a practical framework to improve Texans’ health outcomes while containing long-term public expenditures.
This publication was produced by Rice University’s Baker Institute for Public Policy. Wherever feasible, the material was reviewed by outside experts prior to release. Any errors or omissions are solely the responsibility of the author(s).
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author(s) and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s) and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.


