
Overview
In May 2025, the Make America Healthy Again (MAHA) Commission published its inaugural report, subtitled “Make Our Children Healthy Again”. The document identifies four major drivers of childhood chronic illness: 1) poor diet, 2) aggregation of environmental chemicals, 3) lack of physical activity and chronic stress, and 4) overmedicalization. This initial report was followed in September 2025 by a strategy report providing over 120 recommendations “for executive actions to address the childhood chronic disease crisis through advancing research, realigning incentives, increasing public awareness, and fostering private sector collaboration.”
The MAHA Commission was created under Executive Order 14212, is chaired by Secretary of Health and Human Services (HHS) Robert F. Kennedy, Jr., and includes representation from the highest levels of federal administrative agencies. This commission has significant potential to shape policy and funding at federal and state levels. In January 2026, the HHS and the U.S. Department of Agriculture (USDA) revised the dietary guidelines for Americans, often referred to as the food pyramid, with implications for all publicly funded nutritional programs.
As the MAHA report is being used to inform policy and programmatic changes across the country, a clear understanding of its underlying methods and data sources is essential to assessing its foundation. Given the growing policy relevance, this brief examines the data sources used to support the report and identifies the primary and secondary sources that underpin its findings.
Methods
The report does not describe how the authors identified, curated, or weighted evidence to support its recommendations. To assess the references and data cited in the report, this brief uses the following methodology:
- Unique footnotes were searched via Google Chrome, PubMed, and library databases between Oct. 15 and Dec. 31, 2025. Citations were excluded if they could not be verified by at least two identifiers — authorship, publication location, or year — or if they contained broken hyperlinks.
- Authorship was classified by first-author affiliation as academic, governmental, journalist/press, independent research entity, professional organization, industry, intergovernmental agency, or journal editor. Citations were categorized as research studies, including systematic reviews and meta-analyses; reports; narrative reviews; or press materials. Reviews were classified as narrative if they did not include a search strategy consistent with PRISMA guidelines.
- Data from research studies were classified as primary data if derived from microorganisms, human tissue, clinical samples, or clinical trial data. Existing data generated for other purposes were classified as secondary data sources.
- Administrative oversight of secondary data sources was categorized as governmental (United States), academic, international (foreign government or multination collaboration), nonprofit, private, or professional organization. Governmental data sources were identified by their highest-level agency oversight.
Results
The initial MAHA report included 522 footnotes. After removing duplicates (53) and unverifiable citations (16), 452 citations remained. Of these, 53.1% were prepared by academic authors and 29.2% by governmental bodies. Although 60.8% of references were from authors in the U.S., the report drew from authors in 32 other countries. A full breakdown of the references is available in Appendix 1.
Data Sources
Data sources could not be directly identified from 209 (46.2%) citations including narrative reviews (125; 27.7%) and press releases (24; 5.3%). Primary data were presented in 30 (6.6%) citations. The remaining 213 (47.1%) references identified one or more of 192 unique secondary data sources (median, 1; average, 2.25; range, 1–11).
Table 1 — Administrative Oversight of Secondary Data Sources Cited in ‘Make Our Children Healthy Again’
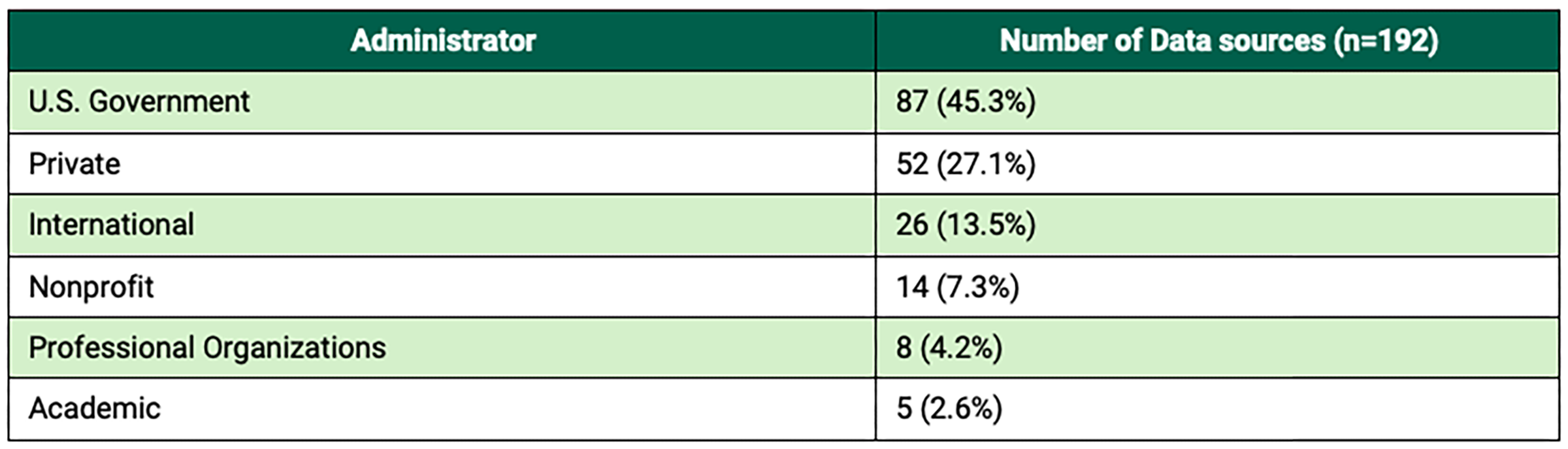
The most frequently identified data sources were literature search engines, including PubMed (n=73), EMBASE (n=29), Web of Science (n=26), PsycINFO (n=21), and Scopus (n=20). PubMed is administered by the National Center for Biotechnology Information (NCBI), funded through HHS, and available without cost to users. The other search engines are administered by private organizations and require a subscription or user fee. These search engines were identified only from systematic literature reviews clearly stating search methods and are therefore likely underrepresented in the report’s citation profile.
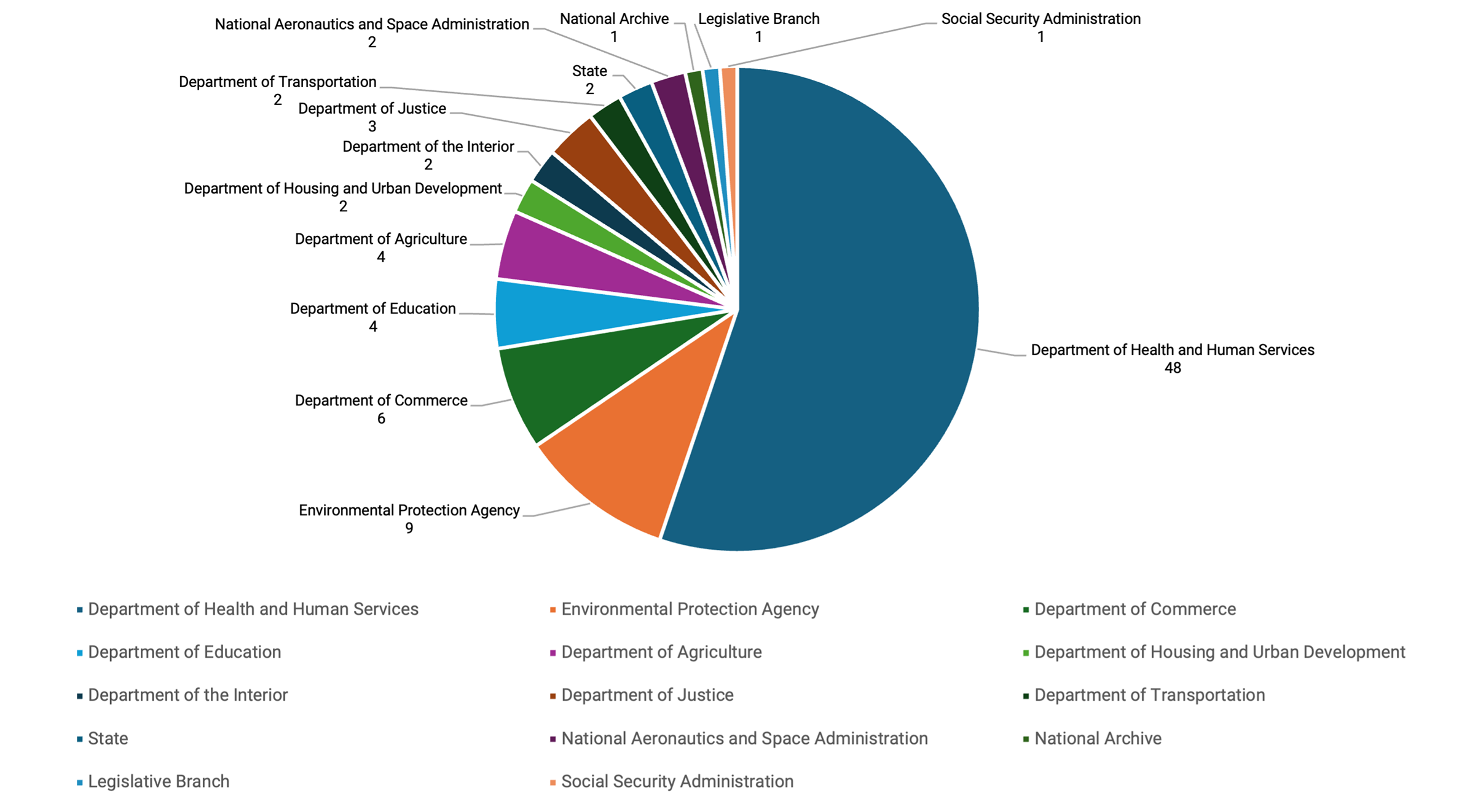
The federal government plays a significant role in administering secondary data sources; only two of the 87 governmental data sources were administered at the state level. Federal secondary data sources came from 12 executive departments and independent agencies, as well as records from the legislative branch. HHS oversees 48 of these data sources (Figure 1). The most cited among them are the National Health and Nutrition Examination Survey (NHANES, 19 citations), the Youth Risk Behavior Surveillance System (12 citations), and the National Survey of Children’s Health (10 citations).
Figure 1 — Governmental Sources of Secondary Data Cited in ‘Make Our Children Healthy Again’
Discussion
Federal guidance has the potential to affect the lives of millions of Americans and is historically held to a high level of scrutiny. The responsibilities of creators of federal guidance are codified in the Information Quality Act (Section 515 of Public Law 106-554), which requires governmental agencies, including those participating in the MAHA Commission, to establish best practices to ensure the “quality, objectivity, utility, and integrity of information” used. These methods are intended to create transparency around the goals of the work, clear steps for evidence inclusion or exclusion, and a framework for assessing the strength of evidence. Established methods also include recognition of interests or biases that may influence interpretation of evidence.
The MAHA report does not include documentation of these steps in its published materials. It does not specify guiding questions, criteria for inclusion or exclusion of research, differentiation in the strength of citations, or disclosure of potential biases or conflicts of interests among authors. These processes may have been conducted but were not made publicly available, which limits transparency as to how the evidence base was constructed.
Federal Context and Information Quality Standards
The MAHA Commission was created under an executive order, and its members identify themselves by leadership positions within federal agencies. As a result, its work operates within existing federal structures, including expectations under the Information Quality Act and related agency guidance. The extent to which those procedures were followed or documented is not addressed in the report’s published materials.
Review of the citations used to support the MAHA report indicates that narrative reviews and press releases were frequently cited in support of claims. Narrative reviews can provide an overview of a topic but are not typically used as a primary sources for guidance development due to limitations in method transparency and potential selection bias. Under HHS’ established guidance, such reviews are categorized among the lower levels of evidence.
Evidence Base and Documentation
Moreover, the MAHA report highlights the role of public institutions in health and science. The MAHA Commission relied on decades of federally funded work to support its foundational premise and identify potential underlying causes. The data referenced from eight cabinet departments, four independent agencies, and two states, exist as a result of public investment. In addition to conducting large-scale data collection that would be difficult for other entities to replicate, the federal government makes many of these resources available at little to no cost to academic and independent researchers.
It is important to note that these data may be affected by ongoing institutional and budgetary changes. In 2025, during the MAHA Commission’s development of its reports, several agencies responsible for generating these datasets experienced personnel and budget reductions.
Notably, NHANES, cited 19 times in the report, is administered by the National Center for Health Statistics within the Centers for Disease Control and Prevention (CDC). This program has collected annual snapshots of health data since 1999. In 2025, the CDC reduced its workforce by around 25%, including personnel supporting NHANES, which may affect the agency’s capacity to maintain data collection at previous levels in the future. Broader reductions in National Institutes of Health (NIH) funding have also impacted the National Center for Biotechnology Information (NCBI), with implications for PubMed, PubChem, ClinicalTrials.gov, and other data repositories. Changes in federal data infrastructure may affect future assessment of policy interventions associated with the MAHA Commission report.
Policy Recommendations
This brief highlights several considerations for policymakers regarding the interpretation and use of findings from the MAHA report. These recommendations focus on ensuring evidence-based decision-making, maintaining research integrity, and supporting the infrastructure needed for effective policy evaluation.
- Treat the Make American Children Healthy Again report as narrative synthesis rather than federal guidance: Any policy derived from its concepts should be independently evaluated for evidentiary support, feasibility, and impact.
- Prioritize unbiased research: Addressing childhood chronic illness requires sustained investment in evidence-based policy development and research methodologies that minimize selection bias and improve reproducibility.
- Protect and strengthen data infrastructure: The ability to evaluate policy outcomes depends on continued support for federal, state, and local data collection and curation systems, including NHANES and related public health datasets.
Appendices
Supporting appendices and additional data are available for download (PDF).
This publication was produced by Rice University’s Baker Institute for Public Policy. Wherever feasible, the material was reviewed by outside experts prior to release. Any errors or omissions are solely the responsibility of the author(s).
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author(s) and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s) and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.


