
Vaccine Exemptions in Texas
Vaccines and vaccine exemptions have become increasingly contentious issues in Texas, with pro- and anti-vaccine groups contesting several vaccine-related bills in the state legislature during the 2017 session. There are two types of exemptions for vaccines: medical and nonmedical. Medical exemptions are issued by a physician, who states that the required vaccine is “medically contraindicated or poses a significant risk to the health and well-being” of a child or someone in their household (TX DSHS 2018a). Examples of medical contraindications include having HIV/AIDS, a compromised immune system, or a life-threatening allergy to any component of the vaccine (CDC 2018a; Rubin et al. 2014). These exemptions, unless otherwise specified, are only valid for one year (TX DSHS 2018a). In contrast, nonmedical exemptions (NMEs) can be requested by a child’s legal guardian who refuses vaccinations based on personal beliefs, including religious and conscientious objections. Unlike medical exemptions, NMEs are valid for two years.
Medical and nonmedical exemptions to vaccine requirements have been permitted in Texas since 1972. In 2003, the state started allowing conscientious exemptions; since then, Texas shows a steady increase in the number of NMEs from 2,314 (0.08% of all students) in 2003-4 to 56,738 in 2017-18 (1.07%) (Matthews and Tan 2018; TX DSHS 2018b).
Vaccine exemptions were a controversial subject during the 85th Texas legislative session in 2017. They were addressed in House Bill 2249 (HB 2249) and House Bill 1124 (HB 1124). While neither of these bills moved forward, the arguments presented by witnesses during the hearings for the bills provide insight into key objections raised by anti-vaccine advocates.
HB 2249, “requirements for and the transparency of epidemiological reports and immunization exemption information and reports,” required the state to report NME rates at the school level, as opposed to the current school district level. This bill received a hearing on April 11, 2017, and was voted out of the committee, although it was not voted out of the chamber by the end of the session (Texas HB 2249 2017). This hearing included 35 witnesses with 12 stating support, 22 opposing the measure, and one witness testifying ‘on’ the bill.
HB 1124, “claiming an exemption from required immunizations for public school students,” intended to make it easier to obtain vaccine NMEs. This bill received a hearing on April 25, 2017, but subsequently died without a committee vote at the end of the session (Texas HB 1124 2017). Twenty-nine witnesses were reported as testified in the hearing, with one stating support, 24 opposing the measure, and the remaining four witnesses testifying ‘on’ the bill. Several witnesses were against school-mandated vaccines as well as the bill itself.
In this issue brief, we describe the key scientific misconceptions presented by vaccine opponents during the witness testimonies for HB 2249 and HB 1124. Transcripts from the two hearings were reviewed, and scientific misconceptions and misinformation were identified, analyzed, and compared to current evidence in the scientific literature. Our results found that vaccine opponents promoted several scientifically questionable ideas, with five major misconceptions identified: 1) vaccines are ineffective, 2) herd immunity is a myth, 3) vaccines ‘shed' and cause the spread of disease, 4) the impacts of vaccine-preventable diseases are minor, and 5) vaccine-exempt children are not spreading disease.
Misconceptions
Five Major Misconceptions About Vaccines
Misconception 1: Vaccines are ineffective.
Reality: Childhood vaccines have high rates of effectiveness.
One common misconception repeated during the witness testimonies was that vaccines are ineffective. On the contrary, most vaccines have extremely high effectiveness rates. The inactivated polio vaccine is 90% effective with two doses and 99-100% effective with three doses (CDC 2018b). The measles, mumps, and rubella (MMR) vaccine is 93% effective with one dose and 97% effective with two doses (CDC 2018c). The diphtheria, tetanus, and pertussis (DTaP) vaccine is 80-90% effective (CDC 2017a). The 1995 implementation of a vaccination program for varicella (chicken pox) reduced incidence, hospitalizations, and deaths by about 90% in the first decade after implementation (Leung, Bialek, and Marin 2015; Lopez et al. 2011; Marin, Zhang, and Seward 2011).
However, witnesses often cited the relatively low effectiveness of the influenza vaccine, with one witness noting that “the 2015-2016 flu shot was only 48% effective” (HB1124-08).1 While the effectiveness of the flu vaccine is low, it is an outlier not the norm (CDC 2018d; Jackson et al. 2017). The influenza virus mutates quickly, and a new version emerges annually. Unfortunately, the strain used for the influenza vaccine is developed months before flu season starts based on researchers’ best predictions, and the strain used for vaccines does not always match the strain that later circulates (WHO 2017). Therefore, effectiveness rates of flu vaccines vary and are not as high as other nonseasonal vaccines, such as those for DTaP and MMR.
Figure 1 — Paralytic Polio Cases Decrease in the U.S. After the Vaccine Was Introduced in 1955 (Shot) and 1961 (Oral)
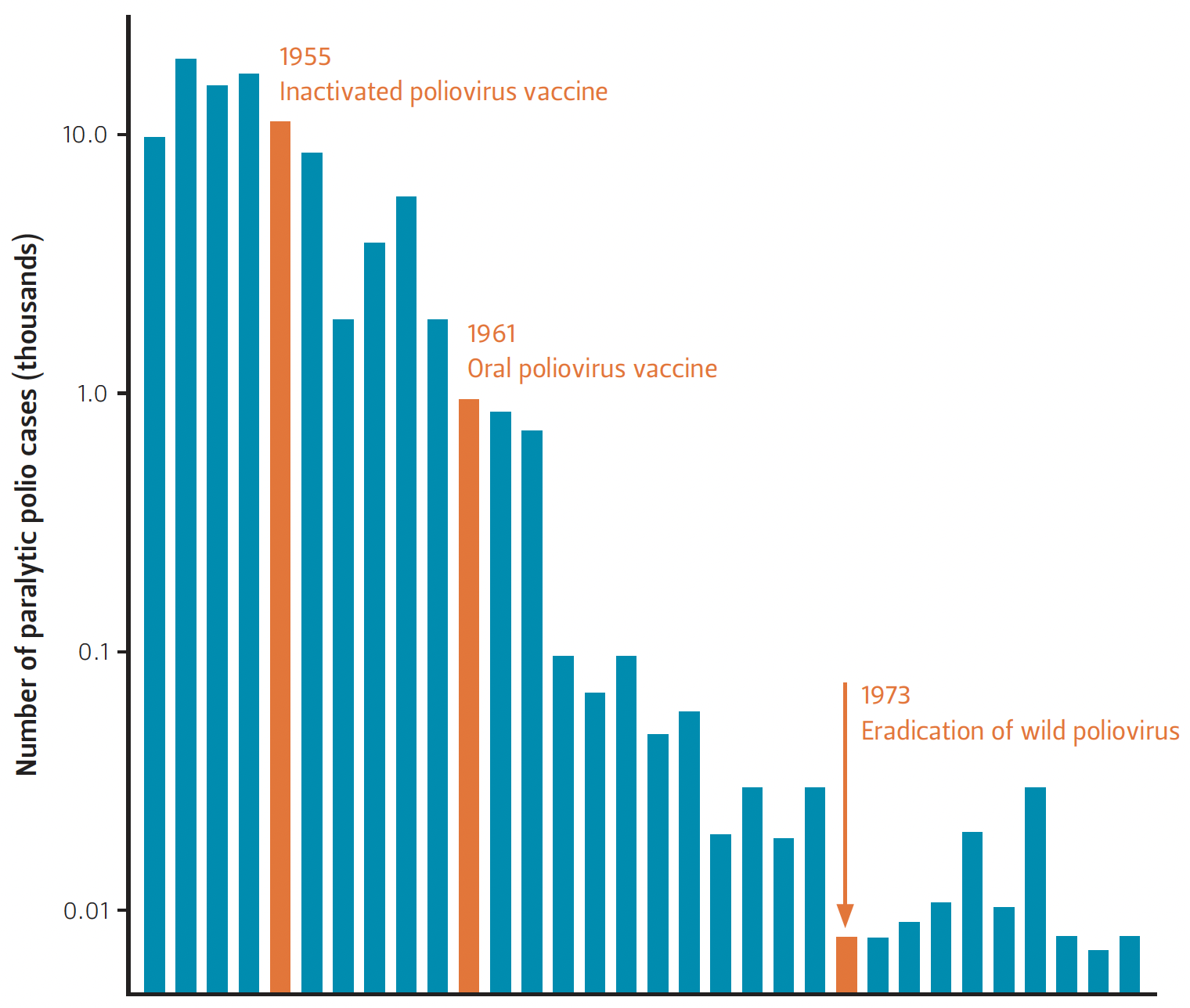
One witness further implied that vaccines can increase disease rates, saying “from the time they started the [polio] vaccine trials, you see a spike up [of the disease]” (HB 2249-08). However, this is false (see Figure 1). Polio epidemiology data show an overall decrease in U.S. paralytic polio cases after both the introduction of the inactivated poliovirus vaccine in 1955 and the oral poliovirus vaccine in 1961 (Nathanson and Kew 2010).
Several witnesses also challenged the effectiveness of vaccines, asserting that “vaccination does not always provide immunity” and “vaccines do not immunize; they interfere with the common immunological response to the respected diseases after subsequent exposure” (HB 2249-05; HB 2249-03). One of these witnesses stated that “two of my children had the full HepB schedule of vaccines, and both them have lab confirmation of zero antibodies to HepB” further claiming that “they are also not immune” (HB 2249-05). Several others were concerned that children who get vaccinated but fail to produce antibodies or gain immunity will become immunocompromised.
These statements highlight a misunderstanding of how vaccines and the immune system work. Vaccines mimic an infection so that the body learns how to fight off a future infection. After vaccination, the body stimulates immune cells (T and B lymphocytes) to mount a specific adaptive immune response against the virus, which helps the body remember how to defend against future infections (Alberts et al. 2015). Scientific research and experiments do not support the belief that vaccination causes immunosuppression. In fact, it is generally recommended that inactivated vaccines can be safely given to immunocompromised patients (Kroger et al. 2011; Sobh and Bonilla 2016).
Misconception 2: Herd immunity is a myth or does not exist.
Reality: Having a significant portion of the public immunized protects people who are immunocompromised, including infants, the elderly, and patients undergoing treatment for immune diseases and cancers.
Herd immunity occurs when the prevalence of immunity in a vaccinated population prevents transmission of infectious agents, thereby offering indirect protection to unvaccinated individuals. Another recurring theme in the witness testimonies is skepticism about herd immunity: “herd immunity is a myth; the math simply does not work” (HB 2249-03). There are two main misconceptions about herd immunity. One misconception is that the concept of herd immunity is invalid; however, numerous studies have shown that the herd effect has helped to reduce rates of disease, including smallpox, pertussis, influenza, and pneumococcal disease (Kim, Johnstone, and Loeb 2011). After the pertussis vaccine became available in the 1940s, a reduction in pertussis was observed not only among vaccinated infants and adults but also among unvaccinated infants because herd immunity reduced the virus's reach (Taranger et al. 2001). Herd immunity also contributed to smallpox reduction in the 1960-70s through a mass vaccination program in endemic countries (Lane 2006). Research on Japanese school children vaccinated for influenza demonstrated protection and reduced influenza mortality among older members of the population. Furthermore, after vaccination requirements were removed and vaccination rates among schoolchildren decreased, excess mortality rates increased (Reichert et al. 2001).
Another misconception about herd immunity is that it is only a theory and does not exist in reality. This argument appeared more frequently during the legislative hearings. One witness alleged that because vaccines wear off, the population does not benefit from herd immunity, claiming that “if all adults in this room right now have not continued to be vaccinated, receive boosters...then we are not all immunized” (HB 1124-08). Similarly, another witness claimed that “vulnerable children...are already surrounded by numerous adults in the school system who don't have the schedule of vaccines that kids get” (HB 2249-13).
It is true that vaccine protection can wane; however, this is why there is a recommended immunization schedule for adults. For instance, a booster for the DTaP vaccine is recommended every 10 years (CDC 2018e). With adherence to the recommended immunization schedule, herd immunity can be maintained, protecting the entire population from disease.
Misconception 3: Vaccines ‘shed’ and cause the spread of disease, endangering the medically fragile.
Reality: Most vaccines do not shed, and there is extremely minimal risk of infection from the few that do shed.
A few witnesses argued that vaccines are harmful to the medically fragile because of ‘vaccine shedding,’ which is the idea that vaccines release the virus into the population. According to one witness, “a recent study suggests that a plausible explanation for whooping cough resurgence is actually asymptomatic transmission from the recently vaccinated,” although they did not share enough detail of the publication for the authors locate the article (HB 2249- 05). This witness concluded that children “who receive live vaccines can put the medically fragile at risk due to shedding.” Another witness, who self-identified as immunocompromised after receiving two bone marrow transplants, said, “every time I have gotten sick, it is because I have been in contact with a child or an adult who is recently vaccinated” (HB 2249-14).
Overall, the occurrence and risks of vaccine shedding are misunderstood. Of the vaccines required by TX DSHS, only the MMR and oral polio vaccine are live attenuated vaccines, which contain weakened forms of the virus. Other vaccines are either inactivated, subunit, or toxoid vaccines, which do not contain live viruses and therefore cannot shed the virus (WHO, n.d.). Shedding from the MMR and the oral polio vaccine is unlikely, and the risk of infection is extremely minimal. Studies show that in the rare case a vaccinated individual is exposed to the mumps virus, vaccination reduces shedding to levels significantly lower than that of infected, unvaccinated individuals. (Fanoy et al. 2011; Gouma et al. 2016).
Yet another witness argued that “polio was eradicated in 1979. Since then every single case of polio has been brought into this world through vaccines” (HB 1124-08). This statement about polio ‘eradication’ is misleading. Since 1979, no polio cases have originated in the United States. However, polio is still present globally. New polio cases since 1979 have been brought into the U.S. by travelers with polio, not through vaccines (CDC 2017b).
Misconception 4: The consequences of vaccine-preventable diseases are minor, while vaccines frequently cause injury and death.
Reality: There are severe consequences of vaccine-preventable diseases, while vaccine risks are extremely minimal.
Vaccine opponents also used the argument that the consequences of vaccine- preventable diseases are relatively insignificant. Measles is often used as an example for this argument. One witness said that “on a local TV channel recently, a M.D. described measles as a lethal disease—how misleading. Historically in the US and other industrialized nations, measles is benign. That means the majority of kids experience no complications, recover efficiently, typically enjoy lifetime of actual immunity as a result” (HB 2249- 03). While measles is no longer endemic in the U.S., the decreased mortality from measles is a result of vaccination. Prior to widespread vaccination, more than half a million cases were reported annually (Table 1). Due to systematic vaccinations, the number of cases has been reduced to only 85 incidents in 2016, with the last reported measles death in the U.S. occurring in 2015 (Fox 2015). Measles infections cause severe complications including bronchitis, pneumonia, encephalitis, and pregnancy problems that led to 11,000 hospitalizations and 123 deaths in the 1989-91 measles resurgence (Mayo Clinic 2018; Orenstein, Papania and Wharton 2004). Similar data on other vaccine-preventable diseases can also be found (Table 1).
Table 1 — Disease Incidence and Vaccination Rates for the U.S. and Texas
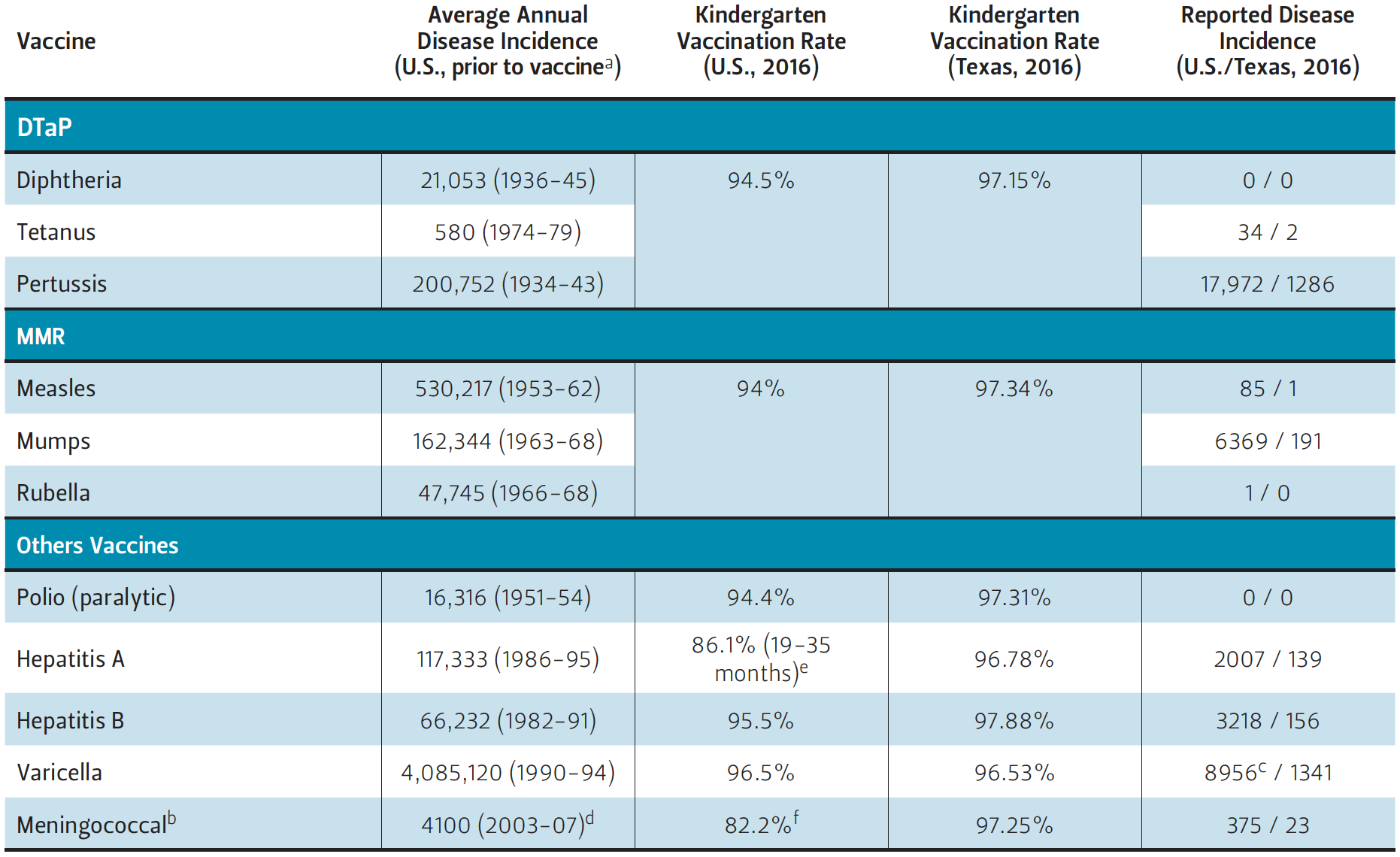
Sources Average Annual Disease Incidence, US Prior to Vaccine: (Roush, et al. 2007), d(Thigpen et al. 2011); Vaccination Rate, U.S. 2016: (CDC 2017c, (e) CDC 2017d, (f) CDC 2018f); Vaccination Rate, Texas 2016: (TX DSHS Immunization Unit 2017); Reported Incidence, U.S. 2016: (CDC 2017e); Reported Incidence, Texas 2016: (TX DSHS 2017).
Witnesses also consistently mentioned that vaccines frequently cause injury and death. In previous years, this discussion focused on autism, but in the 85th legislative session other diseases were highlighted as well, especially Guillain-Barre Syndrome (GBS), an autoimmune disorder. However, scientific research indicates that, with rare exceptions (namely the 1976 swine influenza vaccine), there have only been coincidental associations between vaccines and GBS (Haber et al. 2009; Principi and Esposito 2018). After surveilling more than 3.6 million doses of inactivated influenza vaccine and 250,000 first doses of live attenuated influenza vaccine, no increased risk for GBS, encephalitis, or anaphylaxis was found (Kawai et al. 2014). In contrast, GBS has been associated with Zika and influenza infection (Nóbrega et al. 2018). The risk of vaccine-associated GBS is estimated at less than 1 case per million immunized individuals, which is significantly less than the risk of vaccine-preventable diseases (Principi and Esposito 2018).
Witnesses also expressed fears that vaccines contain toxic ingredients including “aborted fetal tissue, aluminum, mercury, Polysorbate 80” and that “vaccines cause brain inflammation, brain damage, chronic arthritis and a continuing list of autoimmune and neurological disorders” and in some cases, death (HB 2249-04; HB 2249-03). The reason aborted fetal tissue is thought to be a vaccine ingredient is because several vaccines were created using the WI-38 cell line, which was originally developed in 1962 from the lung tissue of an aborted fetus. The WI-38 cell line has been rigorously tested for safety, and the actual cells are not found in vaccines. As a result of using the WI-38 cell line for vaccine development and other medical advancements, an estimated 10.3 million lives have been saved globally (Olshansky and Hayflick 2017).
A few vaccines do include aluminum salts, mercury, and Polysorbate 80 as inactive ingredients (FDA 2018). However, these ingredients have been proven to be safe at the levels used in vaccines. Aluminum levels in infants from vaccine adjuvant and food sources are safely below risk levels (Mitkus et al. 2011). The only vaccine ingredient that contains mercury is thimerosal, a preservative used to prevent the growth of bacteria. Today, thimerosal is not used in any of the required childhood vaccines in the U.S. (CDC 2013). Furthermore, there has been no link discovered between thimerosal and autism (Andrews et al. 2004; Fombonne et al. 2006; Hviidet al. 2003; IOM 2004; Thompson et al. 2007). In addition, Polysorbate 80 is an additive commonly used in food products, including bread, oil, and chocolate. The U.S. Food and Drug Administration (FDA) set the acceptable daily intake (ADI) of polysorbates at 1500 mg per person per day, and an extensive toxicology study conducted in Japan set the ADI at 10 mg per kg body weight per day (Food Safety Commission of Japan 2007). The amount of Polysorbate 80 used in vaccines is significantly less than either of these ADI recommendations. For instance, each dose of the HPV vaccine only has 0.05 mg of Polysorbate 80 (Children’s Hospital of Philadelphia 2018).
One witness suggested that vaccines were linked to sudden infant death syndrome (SIDS), stating that “90% of [SIDS] cases, they happen within 2-7 days of a round of vaccines. There is a lot of evidence of cases that we are losing 3-4,000 infants a year to vaccine fatalities that is a 2 or 3 times as many loss of children’s lives of all ages to all childhood diseases combined in the years leading up to vaccine” (HB 2249-03). There is no scientific basis for the purported link between vaccination and SIDS. The Vaccine Adverse Event Reporting System (VAERS) and the National Academies of Science, Engineering, and Medicine (NASEM) both concluded that trends in the number of SIDS deaths reported to VAERS followed SIDS rates in the general U.S. population, and any association between vaccination and SIDS is coincidental (Silvers et al. 2001; NASEM 2003).
Furthermore, some witnesses drew the conclusion that deaths caused by vaccine injuries outnumber deaths from vaccine-preventable causes. One specifically listed off statistics from unidentified sources, remarking, “in 2014, there was recorded 629 deaths from vaccines; natural causes of those disease were 77 deaths” (HB 1124-08). The witness did not realize that vaccines are the reason so few people are dying of vaccine- preventable diseases (Table 1). Overall, the risks of vaccines are minimal compared to the disease mortality that is prevented by vaccination.
Misconception 5: Vaccine-exempt children are not spreading disease.
Reality: Vaccine outbreaks are primarily occurring among unvaccinated populations.
Several witnesses alleged that children with vaccine exemptions are not responsible for spreading disease. Addressing HB 2249, one witness argued that “the bill makes a misguided presumption that children with vaccine exemptions are responsible for spreading disease, and that vaccinated children are protected and unable to transmit disease” (HB 2249-05). To support this claim, another witness stated that “current outbreaks seem to have occurred a lot among highly vaccinated population” (HB 2249-12). A different witness mentioned that in “the recent mumps outbreak, we wrote to the health department, found out that most of these mumps outbreaks, almost all of the kids were fully vaccinated” (HB 2249-13). Some argued that “exposure to potential pathogens is ubiquitous,” and therefore both “vaccinated and unvaccinated children... develop and spread [diseases] to others” (HB 2249-03).
These ideas are contrary to the scientific literature. In a review of 1416 measles cases, 56.8% had no history of measles vaccination (Phadke et al. 2016). During the five largest U.S. pertussis outbreaks impacting an entire state, 24-45% of affected individuals were unvaccinated or undervaccinated individuals. While there were outbreaks among highly vaccinated populations, these were attributed to waning immunity.
Conclusions and Recommendations
Analysis of the anti-vaccine witness statements presented during the 85th Texas Legislative Session in 2017 revealed five recurring misconceptions: 1) vaccines are ineffective, 2) herd immunity is a myth, 3) vaccines ‘shed' and cause the spread of disease, 4) the impacts of vaccine- preventable diseases are minor, and 5) vaccine-exempt children are not spreading disease. Each of these myths is inaccurate and unscientific. Furthermore, the witnesses failed to use accurate scientific data to justify them. The few witnesses who did try to cite research grossly misunderstood or misinterpreted the data.
Given these misconceptions, there is a clear need to increase the awareness of both policymakers and the general public to the positive impact of vaccines, the negative consequences of an undervaccinated public, and how policies can help influence vaccination rates within Texas. One way is to encourage broad public participation in discussions on vaccines that involve physicians, scientists, parents, and students—especially those who are at-risk by being around undervaccinated children. In addition, scientists and doctors should share and discuss publicly available data and research on vaccines and their impacts on public health.
Without strong public support for vaccines and vaccine research, we run the risk of allowing more people to opt-out for nonmedical reasons, thereby increasing the risk of vaccine-preventable disease and decreasing overall public health. Vaccines are low-cost solutions to often expensive and debilitating illnesses. They reduce the public financial burden and increase public health. They are a critical tool for public health and should be encouraged and promoted by the state legislature by increasing access, not disparaged by allowing myths to perpetuate unchallenged.
References
Alberts. B., et al. 2015. “The Innate and Adaptive Immune Systems.” In Molecular Biology of the Cell, 1297-1342. New York: Garland Science Taylor and Francis Group.
Andrews, N., et al. 2004. “Thimerosal Exposure in Infants and Developmental Disorders: A Retrospective Cohort Study in the United Kingdom Does Not Support a Causal Association.” Pediatrics 114(3): 584:592. https://doi.org/10.1542/peds.2003-1177-L.
Centers for Disease Control and Prevention (CDC). 2013. Understanding Thimerosal, Mercury, and Vaccine Safety. https://www.cdc.gov/vaccines/hcp/conversations/downloads/vacsafe-thimerosal-color-office.pdf.
CDC. 2017a. Pertussis Frequently Asked Questions. https://www.cdc.gov/pertussis/about/faqs.html.
CDC. 2017b. Polio Elimination in the United States. https://www.cdc.gov/polio/us/.
CDC. 2017c. 2016-17 School Vaccination Coverage Report. https://www.cdc.gov/vaccines/imz-managers/coverage/schoolvaxview/data-reports/coverage-reports/2016-17.html.
CDC. 2017d. 2016 Childhood Hepatitis A Vaccination Coverage Report. https://www.cdc.gov/vaccines/imz-managers/coverage/childvaxview/data-reports/hepa/reports/2016.html.
CDC. 2017e. National Notifiable Infectious Diseases and Conditions: United States. https://wonder.cdc.gov/nndss/static/2016/annual/2016-table1.html.
CDC. 2018a. Who Should Not Get Vaccinated with these Vaccines?. https://www.cdc.gov/vaccines/vpd/should-not-vacc.html.
CDC. 2018b. Polio Vaccine Effectiveness and Duration of Protection. https://www.cdc.gov/vaccines/vpd/polio/hcp/effectiveness-duration-protection.html.
CDC. 2018c. Measles Vaccination. https://www.cdc.gov/measles/vaccination.html.
CDC. 2018d. Seasonal Influenza Vaccine Effectiveness, 2004-2018. https://www.cdc.gov/flu/professionals/vaccination/effectiveness-studies.htm.
CDC. 2018e. 2018 Recommended Immunizations for Adults by Age in Easy-to-read Format. https://www.cdc.gov/vaccines/schedules/easy-to-read/adult-easyread.html.
CDC. 2018f. 2016 Adolescent MenACWY Vaccination Coverage Report. https://www.cdc.gov/vaccines/imz-managers/coverage/teenvaxview/data-reports/menacwy/reports/2016.html.
Children’s Hospital of Philadelphia. 2018. Vaccine Ingredients. https://www.chop.edu/centers-programs/vaccine-education-center/vaccine-ingredients.
Fanoy, E. B., et al. 2011. “Transmission of mumps virus from mumps-vaccinated individuals to close contacts.” Vaccine 29(51): 9551–9556. https://doi.org/10.1016/J.VACCINE.2011.09.100.
Fombonne, E., R. Zakarian, A. Bennett, L. Meng, and D. McLean-Heywood. 2006. “Pervasive Developmental Disorders in Montreal, Quebec, Canada: Prevalence and Links With Immunizations.” Pediatrics 118(1): e139–e150. https://doi.org/10.1542/peds.2005-2993.
Food and Drug Administration (FDA). 2018. Vaccines Licensed for Use in the United States. http://www.fda.gov/BiologicsBloodVaccines/Vaccines/ApprovedProducts/ucm093833.htm.
Food Safety Commission of Japan. 2007. “Evaluation Report of Food Additives: Polysorbates.” http://www.fsc.go.jp/english/evaluationreports/foodadditive/polysorbate_report.pdf.
Fox, M. 2015. Washington Woman Is First U.S. Measles Death in 12 Years. https://www.nbcnews.com/health/health-news/woman-dies-measles-first-us-death-12-years-n385946.
Gouma, S., et al. 2016. Severity of mumps disease is related to MMR vaccination status and viral shedding. Vaccine 34(16): 1868–1873. https://doi.org/10.1016/J.VACCINE.2016.02.070.
Haber, P., Sejvar, J., Mikaeloff, Y., and DeStefano, F. 2009. “Vaccines and Guillain-Barré Syndrome.” Drug Safety, 32(4), 309–323. https://doi.org/10.2165/00002018-200932040- 00005.
Hviid, A., M. Stellfeld, J. Wohlfahrt, and M. Melbye. 2003. “Association Between Thimerosal-Containing Vaccine and Autism.” JAMA 290(13): 1763. https://doi.org/10.1001/jama.290.13.1763.
Institute of Medicine (IOM). 2004. Immunization Safety Review: Vaccines and Autism. Washington, D.C.: National Academies Press. https://doi.org/10.17226/10997.
Jackson, M. L., et al. 2017. “Influenza Vaccine Effectiveness in the United States during the 2015–2016 Season.” New England Journal of Medicine 377(6): 534–543. https://doi.org/10.1056/NEJMoa1700153.
Kawai, A. T., et al. 2014. “Absence of associations between influenza vaccines and increased risks of seizures, Guillain- Barré syndrome, encephalitis, or anaphylaxis in the 2012-2013 season.” Pharmacoepidemiology and Drug Safety 23(5): 548–553. https://doi.org/10.1002/pds.3575.
Kim, T. H., J. Johnstone, and M. Loeb. 2011. “Vaccine herd effect.” Scandinavian Journal of Infectious Diseases 43(9): 683–9. https://doi.org/10.3109/00365548.2011.582247.
Kroger, A., C. Sumaya, L. Pickering, and W. Atkinson. 2011. “General Recommendations on Immunization: Recommendations of the Advisory Committee on Immunization Practices (ACIP).” https://www.cdc.gov/mmwr/preview/mmwrhtml/rr6002a1.htm.
Lane, J. M. 2006. “Mass vaccination and surveillance/containment in the eradication of smallpox.” Current Topics in Microbiology and Immunology 304: 17–29. https://doi.org/10.1007/3-540-36583-4_2.
Leung, J., S. R. Bialek, and M. Marin. 2015. “Trends in varicella mortality in the United States: Data from vital statistics and the national surveillance system.” Human Vaccines & Immunotherapeutics 11(3): 662–8. https://doi.org/10.1080/21645515.2015.1008880.
Lopez, A. S., J. Zhang, C. Brown, and S. Bialek. 2011. “Varicella-Related Hospitalizations in the United States, 2000-2006: The 1-Dose Varicella Vaccination Era.” PEDIATRICS 127(2): 238–245. https://doi.org/10.1542/peds.2010-0962.
Marin, M., J. X. Zhang, and J. F. Seward. 2011. “Near Elimination of Varicella Deaths in the US After Implementation of the Vaccination Program.” PEDIATRICS 128(2): 214–220. https://doi.org/10.1542/peds.2010-3385.
Matthews, Kirstin R.W., and Melody T. Tan. 2018. Medical Freedom, Privacy, and Fear of Discrimination: The 2017 Texas Legislative Session Anti-vaccine Arguments. Issue brief no. 10.22.18. Rice University’s Baker Institute for Public Policy, Houston, Texas. https://bit.ly/2q3uNj0.
Mayo Clinic. 2018. Measles. https://www.mayoclinic.org/diseases-conditions/measles/symptoms-causes/syc-20374857.
Mitkus, R. J., et al. 2011. “Updated aluminum pharmacokinetics following infant exposures through diet and vaccination.” Vaccine 29(51): 9538– 9543. https://doi.org/10.1016/J.VACCINE.2011.09.124.
NASEM (The National Academies of Sciences, Engineering, Medicine). 2003. Immunization Safety Review: Vaccinations and Sudden Unexpected Death in Infancy. http://www.nationalacademies.org/hmd/Reports/2003/Immunization-Safety-Review-Vaccinations-and-Sudden-Unexpected-Death-in-Infancy.aspx.
Nathanson, N., and O. M. Kew. 2010. “From emergence to eradication: the epidemiology of poliomyelitis deconstructed.” American Journal of Epidemiology 172(11): 1213–29. https://doi.org/10.1093/aje/kwq320.
Nóbrega, M. E. B., et al. 2018. “Surto de síndrome de Guillain-Barré possivelmente relacionado à infecção prévia pelo vírus Zika, Região Metropolitana do Recife, Pernambuco, Brasil, 2015.” Epidemiologia e Serviços de Saúde 27(2): e2017039. https://doi.org/10.5123/S1679-49742018000200016.
Olshansky, S. J., and L. Hayflick. 2017. “The Role of the WI-38 Cell Strain in Saving Lives and Reducing Morbidity.” AIMS Press 4(2): 127–138. https://doi.org/10.3934/publichealth.2017.2.127.
Orenstein, W. A., M. J. Papania, and M. E. Wharton. 2004. “Measles Elimination in the United States.” The Journal of Infectious Diseases 189(s1): S1–S3. https://doi.org/10.1086/377693.
Phadke, V. K., R. A. Bednarczyk, D. A. Salmon, and S. B. Omer. 2016. “Association Between Vaccine Refusal and Vaccine-Preventable Diseases in the United States: A Review of Measles and Pertussis.” JAMA 315(11): 1149–58. https://doi.org/10.1001/jama.2016.1353.
Principi, N., and S. Esposito. 2018. “Vaccine-preventable diseases, vaccines and Guillain-Barre’ syndrome.” Vaccine. https://doi.org/10.1016/j.vaccine.2018.05.119.
Reichert, T. A., et al. 2001. “The Japanese Experience with Vaccinating Schoolchildren against Influenza.” New England Journal of Medicine 344(12): 889–896. https://doi.org/10.1056/NEJM200103223441204.
Roush, S. W., et al. 2007. “Historical Comparisons of Morbidity and Mortality for Vaccine-Preventable Diseases in the United States.” JAMA 298(18): 2155. https://doi.org/10.1001/jama.298.18.2155.
Rubin, L. G., et al. 2014. “2013 IDSA Clinical Practice Guideline for Vaccination of the Immunocompromised Host.” Clinical Infectious Diseases 58(3): e44–e100. https://doi.org/10.1093/cid/cit684.
Silvers L.E., et al. 2001. “The epidemiology of fatalities reported to the Vaccine Adverse Event Reporting System 1990- 1997.” Pharmacoepidemiology and Drug Safety 10(4): 279-285. https://doi.org/10.1002/pds.619.
Sobh, A., and F. A. Bonilla. 2016. “Vaccination in Primary Immunodeficiency Disorders.” The Journal of Allergy and Clinical Immunology: In Practice 4(6): 1066–1075. https://doi.org/10.1016/J. JAIP.2016.09.012.
Taranger, J., et al. 2001. “Mass Vaccination of Children with Pertussis Toxoid—Decreased Incidence in Both Vaccinated and Nonvaccinated Persons.” Clinical Infectious Diseases 33(7): 1004–1010. https://doi.org/10.1086/322639.
Texas Department of State Health Services (TX DSHS). 2017. Texas Vaccine Preventable Disease Epidemiology Update. https://www.dshs.texas.gov/uploadedFiles/Content/Prevention_and_Preparedness/immunize/TIC%20-%2011-29_10-30_Texas-Vaccine-Preventable-Disease-Epidemiology-Update.pdf.
TX DSHS. 2018a. Exemption Information - School Immunizations. https://www.dshs.texas.gov/immunize/school/exemptions.aspx.
TX DSHS. 2018b. Conscientious Exemptions Data - Vaccination Coverage Levels. https://www.dshs.texas.gov/immunize/coverage/Conscientious-Exemptions-Data.shtm.
TX DSHS Immunization Unit. 2017. 2016-2017 Annual Report of Immunization Status of Students. https://dshs.texas.gov/immunize/coverage/schools/.
Texas HB 2249. 2017. “Relating to requirements for and the transparency of epidemiological reports and immunization exemption information and reports.” https://capitol.texas.gov/tlodocs/85R/billtext/html/SB01010I.htm.
Texas HB 1124. 2017. “Relating to claiming an exemption from required immunizations for public school students.” https://capitol.texas.gov/tlodocs/85R/billtext/html/HB01124I.htm.
Thigpen, M. C., et al. 2011. “Bacterial Meningitis in the United States, 1998– 2007.” New England Journal of Medicine 364(21): 2016–2025. https://doi.org/10.1056/NEJMoa1005384.
Thompson, W. W., et al. 2007. “Early Thimerosal Exposure and Neuropsychological Outcomes at 7 to 10 Years.” New England Journal of Medicine 357(13): 1281–1292. https://doi.org/10.1056/NEJMoa071434.
WHO (World Health Organization). n.d. Module 2: Types of vaccine and adverse reaction. http://www.who.int/vaccine_safety/initiative/tech_support/Part-2.pdf.
WHO. 2017. Influenza. http://www.who.int/biologicals/vaccines/influenza/en/.
Acknowledgments
The authors would like to acknowledge the help of SuJin Kang and Richard Bui, who reviewed videos and transcripts from the 2017 hearings and conducted literature reviews. We would also like to acknowledge Sharon Tsao and Jonathan Picker, who edited the manuscript.
Endnotes
1. Witnesses were de-identified and numbered based on the hearing they participated in. For full hearing testimonies see (Texas HB 2249) and (Texas HB 1122).
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s), and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.


