
Introduction
Access to health care providers continues to be a problem for children in Texas. According to the Center for Public Policy Priorities, 1 out of 8 children were uninsured in 2013, despite health insurance programs for low-income children, such as Medicaid and the Children’s Health Insurance Program (CHIP).1 Additionally, practical barriers—such as inability of parents to miss work or travel long distances to a health care provider—create hindrances to health care access. Medical care for children is important because early recognition and treatment of chronic diseases decreases morbidity and mortality in adulthood.2 In addition, early interventions for chronic conditions decrease costs to the health care system. For instance, it is estimated that a 1 percent reduction in the number of overweight and obese adolescents could reduce medical costs by over $586 million.3
One solution to increasing health care access for children is school-based health centers (SBHC). An SBHC is run very much like a traditional doctor’s office, with the exception that many are staffed by nurse practitioners. They are designed to provide primary care and/or mental health services within the school. SBHCs were first conceived in the 1970s as a way to reduce health-related absences and improve access to care for underserved children. Since the 1970s, nearly 2,000 SBHCs have become operational in the United States, 85 of which are in Texas. SBHCs have been shown to improve health management for students with asthma and diabetes, and increase preventative care and immunizations.4 In recognition of the value of SBHCs, the Affordable Care Act (ACA) appropriated $200 million toward the improvement and expansion of SBHCs between 2010 and 2013. School-based health centers are typically funded through a mix of private, government, in-kind, foundation, and Medicaid dollars. However, funding is not always stable and the operational and staff costs of running the clinics can range from $116,000 to $402,500 depending on the services provided.5
A less expensive alternative to SBHCs is school nurses. School nurse programs pre-date SBHCs and have existed since the early 1900s. School nurses can manage chronic conditions, perform health screenings and immunizations, provide health education, and triage acute illnesses, which together take care of the majority of health-related problems for children.6 Similar to the benefits of SBHCs, school nurse programs have demonstrated reduced absences and impact health outcomes in certain chronic diseases, such as obesity and asthma. The disadvantage of the school nurse program compared to the SBHC is that nurses are not licensed to diagnose and treat medical conditions, and therefore a referral to a higher licensed provider, such as a nurse practitioner or physician, would be required at times. Funding can also be challenging because as public school financing becomes tighter, school nurses are often cut first, leaving some schools without a school nurse and others with a nurse only a day or two a week.
Tele-health in schools may be the answer to limited resources and a need to increase health care access for children. Tele-health refers to the use of information and communications technology to deliver a broad range of health care services remotely, including clinical care, health education, and counseling. Based on our experience, the telecommunications equipment needed in a school clinic can be as simple as a computer, Web cam, encrypted software, electronic stethoscope, and video otoscope. Therefore, the start-up costs of a school tele-health program could be relatively low.
Tele-health in Schools
Tele-health has been used in a few schools nationwide. For example, a tele-health program in Rochester, New York, Health-e-Access (HeA), provided health care in over 60 childcare and elementary school settings.7 The program included 70 primary care clinicians who diagnosed and treated acute and chronic illnesses. The program demonstrated a 63 percent reduction in absences due to illness and a 22.2 percent reduction in emergency department (ED) utilization. The utilization of acute health care services was 3.5 percent higher for children with access than for those without.8 Moreover, 95 percent of parents whose children participated in the HeA have stated they would choose a child care program with telemedicine over one without it, and parents estimated an average of 4.5 hours was saved compared to an in-person health care visit.9 The program cost approximately $12 million to develop and evaluate, and is sustained through health insurance reimbursements for physician services.
TeleKidcare, located in Kansas, utilized tele-health to connect four elementary schools with physicians at the local academic medical center.10 Each school had a school nurse who utilized a PC-based videoconferencing system, electronic stethoscope, and digital otoscope to facilitate the tele-health consult with the physician.11 The program’s success in reducing absenteeism and improving parent satisfaction mirrored that of Health-e-Access. TeleKidcare was recognized as a Best Practices Initiative by the U.S. Department of Health and Human Services.12
Most of the tele-health programs in schools serve the intended purpose of increasing student access to health care, but do so at a cost substantially higher than school nurse programs. Physician services represent the highest health care labor cost; when physicians are substituted with nurse practitioners, the labor cost dips, but it is still significant. Moreover, models that rely on reimbursements from health insurance companies for episodic visits may be difficult to sustain when the patients the clinics aim to serve are underinsured or uninsured. Yet the costs may be well worth it in rural communities where a pediatrician is not in close proximity. In those instances, using tele-health to connect a child to a physician is a valuable and much needed investment.
On the other hand, utilizing tele-health in urban schools may not be the most cost-effective model. Children in urban areas do have physical barriers to access, such as the inability of parents to miss work and take their child to the doctor. However, coordinating care with local pediatricians who have non-traditional clinic hours may prove just as effective. Also, most school-aged children, who otherwise have some access to a primary care physician, present to the school clinic with ailments that could be managed through interventions by the school nurse. School nurses also coordinate with local physicians to address chronic disease management and facilitate continuity of care with the physician, which is also appropriate in urban settings.
Even if tele-health may not be the most appropriate mechanism to connect children with physicians in urban areas, it can be utilized to increase access to existing school nurses. There is no current model describing a tele-health system that increases access to school nurses, and this issue brief aims to describe a hypothetical model that could be adopted in urban cities, such as Houston, Texas.
Tele-health Model
An urban school district that has funding for some school nurses, but not enough to permit continuous coverage during the school week for all schools in the district, may benefit from a tele-health model that maximizes access to school nurses. For example, a nurse who usually travels to three different elementary schools each week to provide care could still be physically present at those schools the same number of days, while also available to consult with students from her other assigned schools via tele-health. Such an arrangement would amount to five days a week continuous coverage for those three schools.
In Texas, tele-health is defined as a health service delivered by a licensed or certified health professional acting within the scope of the health professional's license or certification who does not perform a telemedicine medical service and that requires the use of advanced telecommunications technology, other than telephone or facsimile technology.13 In other words, health services provided via telecommunications by licensed health care professionals who are not physicians are defined as tele-health encounters in Texas. The same requirements of informed consent and patient confidentiality that apply in traditional medical settings also apply in tele-health encounters.14,15
The remaining regulations regarding tele-health seem to focus primarily on telecommunications with physicians, which the Texas statute denotes as “telemedicine.” For example, there is a requirement for a patient presenter, i.e., an individual physically present with the patient who can assist the distant provider with the examination during telemedicine encounters. The presenter must be licensed or certified in Texas to perform health care services or be a qualified mental health professional for community services, and be delegated only tasks and activities within the scope of the presenter's licensure or certification by the physician. There is not an analogous provision in the statutes regarding tele-health, which at least indicates there is not a legal requirement to have a licensed health professional be the patient presenter when the distant site provider is not a physician. Instead, it may be possible to train school office staff or volunteers (with the applicable confidentiality agreements in place) to use tele-health equipment to present the students to the off-site nurse. This model would allow school nurses to be physically present at a school they normally travel to one day a week, while also consult with students from their other schools. Maximizing the accessibility to school nurses allows for continuity of care for the students, and could decrease inappropriate referrals home or to the emergency department by school staff.
Tele-health Equipment
The equipment requirements will vary greatly between programs and depend heavily upon resources and objectives. Minimum requirements include a computer with video conferencing capability and an Internet connection that supports a high bandwidth connection. All electronic communications would need to be on secure, encrypted servers. A reliable and secure system for storing patient information is also essential. Whether additional equipment is needed depends on what the school nurse typically uses on a routine basis, and whether the school district wants to have the capability to use the tele-health equipment to connect with physicians. Table 1 outlines the price ranges and possibilities for equipment for a school tele-health program.
Table 1 — Estimated Cost—Telemedicine Equipment
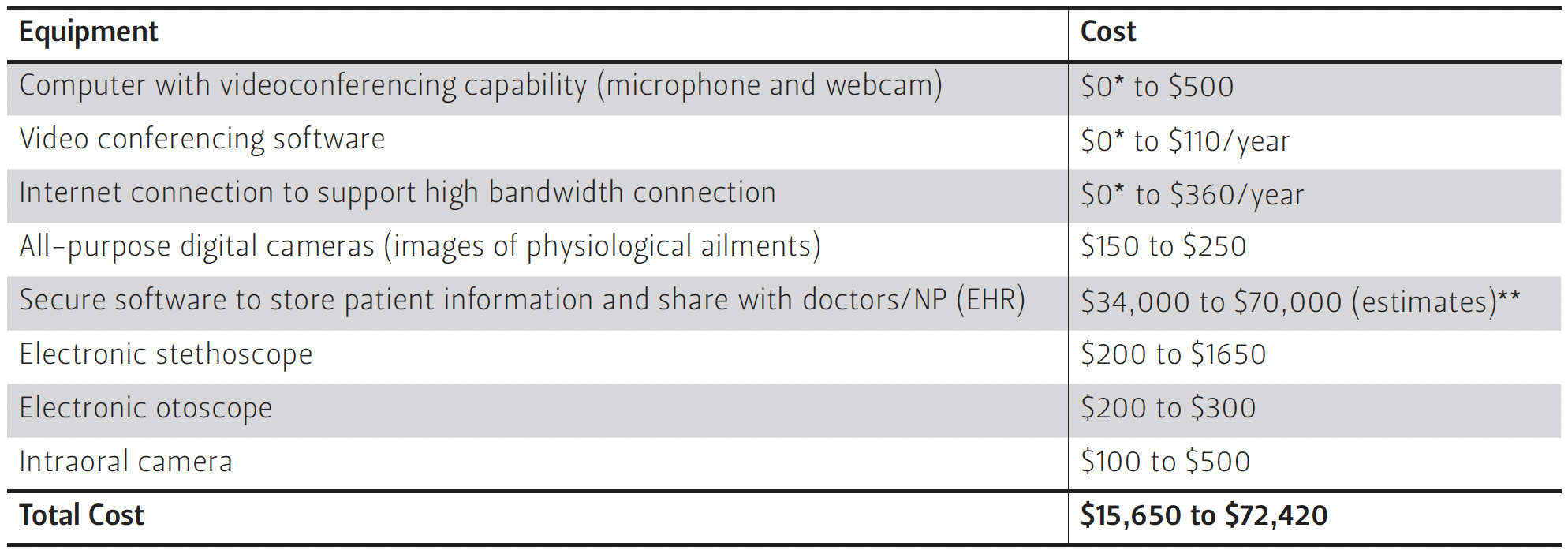
**Additional EHR resources can be found at http://www.healthit.gov/providers-professionals/faqs/how-much-going-cost-me.
Staffing and Licensure
A nurse participating in this proposed tele-health model would have to be a registered nurse (RN). RNs must have at least an associate’s degree (two years of post-secondary school) and complete the required educational programs to be licensed to practice the vocation of nursing in the state of Texas.16 An RN can administer medications, develop nursing care plans, and can observe, assess, and provide care and counsel to patients.17 Moreover, the medical director of the school-based program can delegate tasks to the RNs and develop protocols for triaging and addressing acute and chronic illness. RNs can also provide health education interventions for injuries, some emergencies, communicable diseases, obesity, substance use and abuse, adolescent pregnancy, mental health, dental disease, nutrition, and sexually transmitted infections.18 However, prescriptive authority, medical diagnosis, and treatment plans cannot be delegated to an RN. Therefore, students would have to be referred for conditions requiring treatment.19
Cost
Ideally, the only cost for a school district would be the tele-health equipment, which may be much lower than our estimated costs if the district is currently using electronic health records (EHR) in its school health program. Moreover, the cost of EHRs varies so widely that there are likely less expensive EHRs than those we quote. Staffing is the other major cost of any tele-health program. Our model proposes utilizing the existing school nurse staff and training school staff to be patient presenters, and therefore would not require additional staff. However, we made the assumption that the school nurses would have the capacity to consult with other students via tele-health while also being physically present at another school. It is possible there are schools that have a high demand for the school nurse so there is not additional capacity to see students via tele-health. For those schools, additional nurses may be required, which would increase the cost.
Yet even with additional staffing requirements at certain schools, the net cost savings for not needing a nurse for every school, as well as the net benefit to society, makes this model a viable option. It has been reported that school nursing services can generate a net benefit of $98.2 million to society, with program benefits measured by savings in medical procedure costs, teachers’ productivity loss costs associated with addressing students’ health issues, and parents’ productivity loss costs associated with student early dismissal and medication administration.20 Thus for every dollar invested into a school nurse program, society would gain $2.20.
Conclusion
Increasing children’s access to a primary care physician is an important component of ensuring a healthier generation of children. However, tele-medicine in schools may not be the most cost-effective strategy for increasing access for children, particularly in urban areas. Tele-health, on the other hand, may optimize existing school nurse programs and can still lead to improved health for children. Moreover, by maximizing the use of school nurses, only the students who need evaluation by a higher licensed provider will be referred, which reduces cost on the overburdened U.S. health care system. School nurse programs have similar success in reducing the use of emergency departments, improving the management of chronic diseases, and reducing absenteeism. Therefore, the benefits of a school nurse tele-health model could closely compare to a school telemedicine model.
There will never be a “one-size fits all” solution to the U.S. health care crisis, but at the very least, tele-health may be a cost-effective option to increase access to a health care professional for the children who need it the most.
Endnotes
1. Center for Public Policy Priorities, Texas Kids Count Project, accessed May 26, 2015, http://forabettertexas.org/kidscount.html.
2. Michele Cecchini, Franco Sassi, Jeremy A. Lauer, Yong Y. Lee, Veronica Guajardo-Barron, and Daniel Chisholm, "Tackling of Unhealthy Diets, Physical Inactivity, and Obesity:Health Effects and Cost-effectiveness," Lancet 376, no. 9754 (November 2010): 1775-1784, doi:10.1016/S0140-6736(10)61514-0.
3. Li Y. Wang, Maxine Denniston, Sarah Lee, Deborah Galuska, and Richard Lowry, "Long-term Health and Economic Impact of Preventing and Reducing Overweight and Obesity in Adolescence," Journal of Adolescent Health 46 (2010): 467-473, doi:10.1016/j.jadohealth.2009.11.204.
4. Jessica Strolin-Goltzman, Amanda Sisselman, Kelly Melekis, and Charles Auerbach, “Understanding the Relationship between School-Based Health Center Use, School Connection, and Academic Performance,” Health & Social Work 39 (2014): 83-91.
5. Robert J. Nystrom and Adriana Prata, “Planning and Sustaining a School-Based Health Center: Cost and Revenue Findings from Oregon,” Public Health Reports 123 (2008): 751-760.
6. American Academy of Pediatrics Council on School Health, “Role of the School Nurse in Providing School Health Services,” Pediatrics 121 (2008): 1052-1056, doi:10.1542/peds.2008-0382.
7. Kenneth M. McConnochie, Nancy E. Wood, Neil Herendeen, Phillip K. Ng, et al., “Acute Illness Care Patterns Change with Use of Telemedicine,” Pediatrics 123 (2009): e989-e995.
8. Ibid.
9. Ibid.
10. Pamela Whitten and David J. Cook, “School-Based Telemedicine: Using Technology to Bring Health Care to Inner-City Children,” Journal of Telemedicine and Telecare 5 Suppl (1999): S23-5.
11. Ibid.
12. Michael Mackert and Pamela Whitten, “Successful Adoption of a School-Based Telemedicine System,” Journal of School Health 77 (2007): 327-330.
13. Tex. Gov. Code §531.001(7).
14. Tex. Occ. Code §111.002.
15. Tex. Occ. Code §111.003.
16. Tex. Occ. Code §301.157.
17. Tex. Occ. Code §301.002(2).
18. American Academy of Pediatrics, “Role of the School Nurse in Providing School Health Services,” Pediatrics 121 (2008):1052-1056.
19. Tex. Occ. Code §301.002.
20. Li Yan Wang, Mary Vernon-Smiley, Mary Ann Gapinski, Marie Desisto, Erin Maughan, and Anne Sheetz, “Cost-Benefit Study of School Nursing Services,” JAMA Pediatrics, doi:10.1001/jamapediatrics.2013.5441.
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s), and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.

