
Health equity means that there are widespread, systemic policies and programs in place to ensure that everyone has equal opportunities to access health care and health-related resources. Unfortunately, this is not always the case and as a result, racial and ethnic minority groups are often disproportionately affected by disease, including COVID-19. Since the beginning of the pandemic, the light at the end of the tunnel has always been herd immunity, obtainable through widespread access to a vaccine. As federal, state, and local vaccination efforts progress, many cases and deaths will be prevented. However, some states still face challenges with racial and ethnic disparities in COVID-19 vaccine distribution, and Texas is one of them. Below we identify the disparities in Texas, offer explanations for the disparities, and make recommendations to prevent this from recurring in any subsequent public health event.
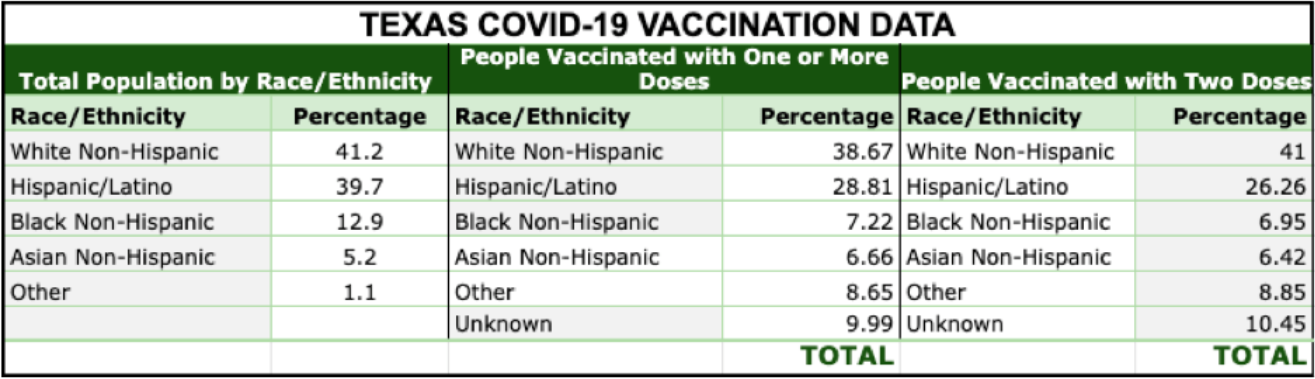
The chart below shows the rate of vaccination by race/ethnicity compared to the share of the population for each group as of April 30, 2021. In an equitable system, we would expect the rates of vaccination and shares of population to line up. In Texas, they do not.
Figure 1 — The Rate of Vaccination by Race/Ethnicity
Why do these disparities exist? We suggest they are due primarily to differences in access to vaccines. In the early months of the roll-out, vaccines were in short supply and groups were pitted against one another in seeking access. The location of vaccination sites, an internet-dependent appointment system, and transportation inequities created barriers to access that were especially challenging for non-White populations. The earliest doses were available through hospital systems. After vaccinating hospital staff, they offered vaccines to established patients. This placed Black and Hispanic populations at a disadvantage because they are less likely to have established relationships with hospitals since they are more likely to be uninsured than Whites.
Even after vaccines became available outside of hospitals in community-based sites, technology and transportation barriers persisted for non-White populations. For those without devices, reliable connections, and the time to search, the opportunity to get an appointment was limited. Most vaccine appointments are secured electronically, and people spent hours searching for openings when appointments were scarce during the initial phase of the roll-out. Black and Hispanic Texans are more likely to lack internet access than White Texans (1). Further, even if someone schedules a vaccination appointment, there may be logistical issues to keeping the appointment. Low-income workers are less likely to have paid time off from work, and people of color are more likely to be paid poverty-level wages. One study showed that people of color are less likely to have workplace flexibility, with only 25% of Latino and 43% of Black workers having access to paid parental leave compared to 50% of White workers. Furthermore, data shows that Black residents may have to travel further for vaccines, which can deter making appointments in the first place. Transportation may be another hurdle to keeping an appointment, particularly for those who don’t own vehicles (drive-through sites may not accept walk-ups) or live near public transportation. A 2017 survey found that Blacks were the least likely of any racial group in America to own a vehicle. Of the remaining options, ride sharing, such as Uber or Lyft, can be expensive, and even public transportation can be a difficult option, due to an increased chance of a COVID-19 exposure.
How might we avoid these inequities in the future? First, we should approach vaccine distribution from a public health perspective and plan accordingly. As is often the case in the U.S., we view health through the lens of health care and disregard (and underfund) the public health infrastructure that exists for large-scale public health events like pandemics. Had we engaged our public health system first, this likely would have resulted in an earlier concerted effort to make vaccines available to communities with the greatest need, based on epidemiological data, rather than relying on hospitals as the primary sites. For example, after the Houston Health Department began receiving vaccines, they developed a strategy for targeted vaccination efforts based on priority zip codes identified using the CDC’s COVID Community Vulnerability Index. Second, by adopting a public health perspective, we would implement a multimodal approach to schedule vaccination appointments appropriate for all populations, including by phone and through public health and community outreach, rather than relying on hospital systems. Lastly, we would address the underlying social and economic conditions that put Black and Hispanic populations at a disadvantage in the face of pandemics, hurricanes, winter storms, and other large disasters. This requires a reimagining of our investments in public goods such as community health.
Ultimately, we believe there is a moral and ethical obligation for the government and the health sector to make sure that everyone gets a fair shot at a healthy life. With more intentionality to the issue of equity, we can do better next time.
Reference
1. Census Bureau ACS 5-Year Survey (2015-2019). Estimated percent of people in (race/ethnicity) households that do not have an internet subscription between 2015-2019 [Map]. PolicyMap. https://plcy.mp/wPgMWFC.
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s), and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.

