
Introduction
The COVID-19 pandemic resulted in widespread suspension of normal commerce and education with massive economic challenges for individuals, industries and governments. In the two years since the initial business and school closures of early 2020, the economic and social impacts have lingered. Now, with policies that could relax childhood immunization requirements emerging across the United States, it is crucial that we remember both the human toll and the economic devastation of COVID-19. It is also critical to consider the financial implications for potential outbreaks of any vaccine-preventable disease. Addressing personal, health care system and government costs of medical decisions is difficult in the United States because our system is disjointed and complex. As a result, many health policy decisions are made with limited information about the economic consequences. However, carefully exploring costs, in combination with data such as case numbers and outcomes, has the potential to improve our health care policy decision-making.[1]
This issue brief analyzes the potential economic impacts of relaxing vaccination requirements for children. Using measles as a test case, existing outbreak data is applied to a decision analytic model to evaluate the short-term impact of an outbreak on the public budget. The findings reveal that as immunization rates decline, the costs of an outbreak increase.
Background
Vaccines have protected children for over 50 years, reducing death and suffering for hundreds of millions of people across the world. In 2022, the Centers for Disease Control and Prevention (CDC), in collaboration with multiple professional bodies, recommended vaccinations against 16 communicable diseases starting immediately after birth and continuing through adulthood, with the majority of individual vaccine doses given in the first five years of life.[2] These kinds of early childhood vaccinations are an essential reason why diseases that used to be common — including polio, measles and diphtheria — are no longer prevalent.
In the United States, high rates of childhood vaccination are achieved by requiring proof of vaccination for children attending licensed childcare and publicly funded education centers.[3] However, policies that make it easier to obtain vaccine exemptions for medical, religious or philosophical circumstances are associated with lower kindergarten immunization rates.[4] In Texas, for example, individual schools and school districts reported kindergarten vaccination rates as high as 99% and as low as 33% for the 2020-2021 academic year.[5]
The success of U.S. immunization programs has meant that parents of young children and many members of the medical community have little experience with the life-threatening consequences of childhood diseases such as measles, whooping cough and polio. As the collective memory of these diseases fades, disproportionate and mostly unfounded concerns over potential vaccine-related toxicities have been growing. In addition, anti-vaccine groups and individuals have preyed upon vaccine fears for personal and political gain. As a result, there are heightened rates of vaccine refusal and hesitancy in the United States, as well as lowered immunization rates and new outbreaks of previously well-controlled diseases.
Vaccines exist at the intersection of personal and public health. A vaccinated individual receives beneficial personal protection (despite experiencing potential side effects) and also imparts protection to their local community by preventing the spread of infection to others. The debate between personal choice and public health often concentrates on health risks such as the number of cases per population, fatalities related to the disease in question and physical symptoms of the illness versus potential toxicities of the vaccine. There is no disputing the importance of these issues in informing policies; our recent experience with COVID-19 demonstrates that outbreaks of communicable diseases have dire consequences.
The COVID-19 pandemic led to a dramatic loss of life and unprecedented economic and social disruptions. As new policies promoting the relaxation of childhood immunization requirements come to the fore in Texas and the nation, it is essential to consider the consequences of future outbreaks — including the potential economic costs.
Potential Costs of Lower Vaccination Rates
Studies that predict costs associated with vaccines most often consider the costs and benefits of introducing a new vaccine or a new program to increase vaccination rates.[6] However, in the United States, vaccine policies and delivery infrastructure already exist, and an alternative approach is needed to predict the potential economic impacts of relaxing vaccination requirements. To that end, this paper uses existing outbreak data to consider the short-term impact of a future outbreak on the public budget — especially as vaccination rates across the United States decline. To understand the costs, a decision analytic model was developed that represents a childhood population under varied vaccination rates and outbreak conditions. This brief focuses on a single-year’s costs that would affect the Texas state budget.
Model Inputs
Measles was used as a test case for a new model of outbreak costs, as it is one of the most contagious yet preventable childhood illnesses.[7] Prior to the advent of the measles vaccine in 1963, approximately 3 million people in the United States were infected, resulting in 48,000 hospitalizations and approximately 500 deaths annually.[8] In contrast, there were only 13 cases of measles reported in 2022 across the entire nation. Anti-vaccine activists have long targeted the measles-mumps-rubella (MMR) vaccine, spreading misinformation about its safety. Their efforts have resulted in lower vaccination rates — for measles as well as other diseases.[9]
In the decade prior to the COVID-19 pandemic, the United States, European nations and numerous low- and middle-income countries were subject to measles outbreaks attributed to communities with particularly low immunization rates and incidents of international travel to areas with outbreaks.[10] In 2019, an unvaccinated child returned from international travel to their home in Clark County, Oregon, a community where only 78% of children over the age of six had received the recommended two MMR doses.[11] As a result, 74 people contracted measles, 73% of whom were children under the age of 10. The costs of this outbreak were estimated to be more than $3.4 million, with $2.3 million attributed to public health efforts to identify and contain further spread of the disease.
Using measles as a test case, our model was developed with data sources that measure state population, the risk of exposure and illness, and state-related costs for measles (Table 1). We isolated the model to look at children from birth to 17 years old, since vaccinations are required and recorded for school enrollment in this age category. In addition, children are most directly affected by measles infections. The established practice is to give the first MMR dose between 12 and 18 months of age and the second between four and six years of age. Infants remain a vulnerable, unvaccinated group.
During the 2019-2020 school year, 97% of Texas kindergarteners had received both doses of MMR, which we used for the upper range of the model. This rate declined to 94% for the 2021-22 school year, with individual schools reporting rates ranging from 33% to 100% of incoming kindergarteners.[12] No further measles vaccinations are recommended in childhood, so we assumed that vaccination rates at kindergarten enrollment would stay the same through age 17. Our model assumed each age cohort under six (less than one year, one year, two years, three years, four years and five years old) made up approximately 5% of the total childhood population, and the remaining 70% were between six and 17 years old.[13]
Table 1: Probabilities and Cost Inputs (in 2021 US$)
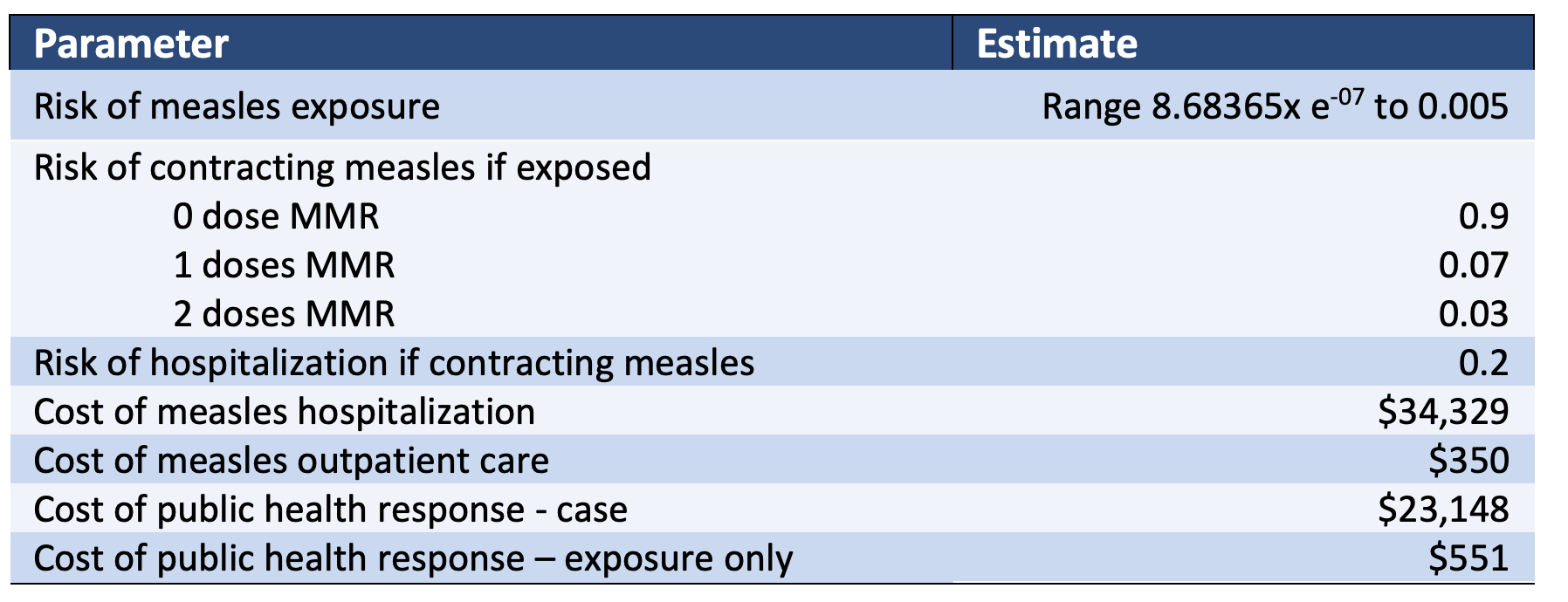
The second set of data used in the model measured the estimated likelihood of a child being exposed to measles. Typically, this likelihood is extremely low. Most outbreaks in the United States start with exposure during travel.[14] Once actual cases exist within a community, the risk of exposure naturally increases. We created a range of probabilities of exposure using global case rates. This included reports from years without any outbreaks in the United States, as well as reports from other countries with low vaccination rates that did experience outbreaks. Once exposed to a case of measles, an individual child’s likelihood of contracting the illness is influenced by their protection through previous MMR doses. If infected, some children will be severely ill and need inpatient hospital care, while others can be cared for at home.
Finally, we incorporated data measuring state-incurred costs during an outbreak including costs for public health responses and medical care for children covered by state-funded health care programs. Public health response costs include actions taken by local and state health departments to contain the disease via contact tracing and diagnostic testing for those exposed. Medical care costs include inpatient hospital stays and pediatrician visits for children who receive medical coverage through state-funded programs. Approximately 48.6% of children in Texas are covered by commercial insurers, 38.6% by state and federally funded Medicaid or Children’s Health Insurance Program (CHIP) programs, and the remaining 12.8% have no insurance coverage.[15] We combined children without insurance and those covered by Medicaid/CHIP for this model, assuming that the state will indirectly supplement their medical costs through payments to hospitals for unfunded care.
Model Results
In this model, the average cost to the state per child increases with both an increase in probability of exposure to measles and a declining vaccination rate (Figures 1 and 2). Because infants are unvaccinated, there will always be a possibility of measles outbreaks. When cases in the community exist, the impact of vaccination on costs becomes apparent. An inflection point of more dramatic increases in costs occurs when an individual’s probability of exposure to measles reaches 0.0005, a rate that represents one case in a community of 2,000 people.
Figure 1: Average Medical Cost of Measles Per Child Increases as the Percent Immunization Rate Decreases
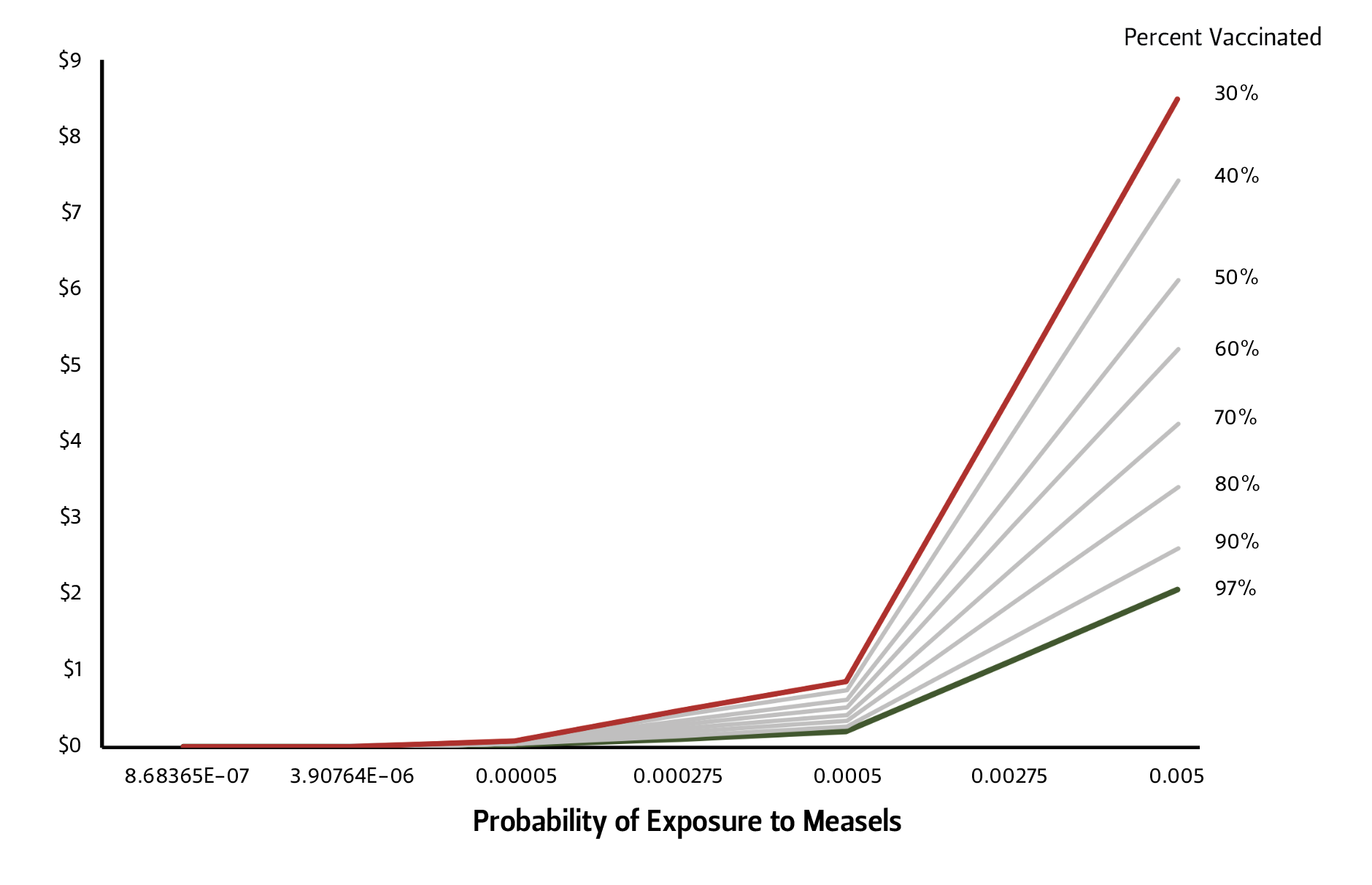
Figure 2: Average Public Health Cost of Measles Per Child Increases as the Percent Immunization Rate Decreases
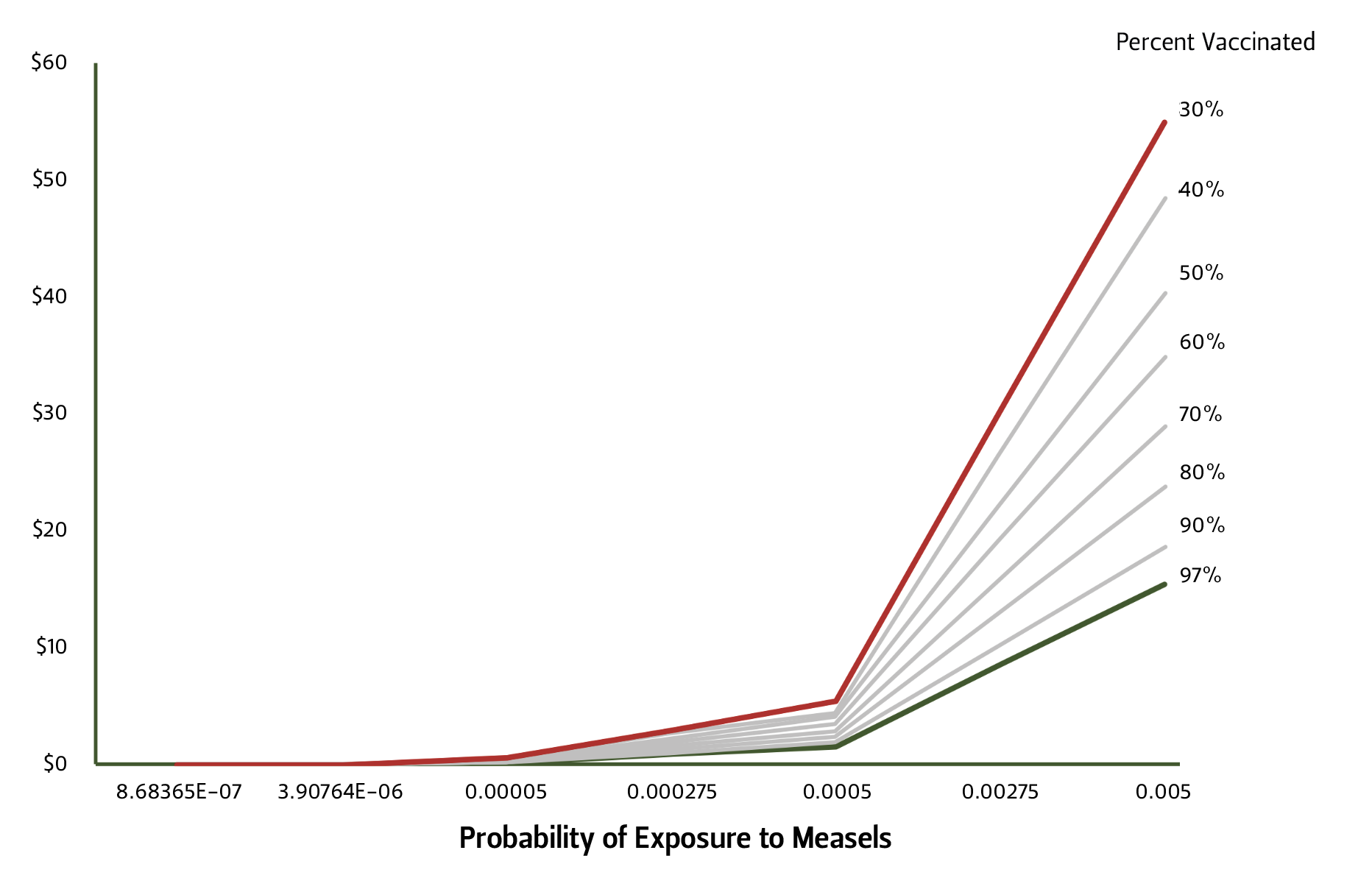
Comparing communities with 30% versus 97% immunization rates, average medical care costs per child and average public health response costs per child are four times and 3.5 times greater, respectively. When there is a low likelihood of measles exposure, the differential between these communities is pennies per child. However, if an outbreak occurs, the cost difference grows to $6.41 per child for medical care and $39.41 per child for the public health response.
The public health response costs per child can range 6.2 to 7.8 times higher than medical care costs per child. One reason for this difference is that we only included medical costs for children whose medical services were funded through state-supporting programs, whereas public health reporting is required for any case or exposure, regardless of medical coverage. A second reason for this difference is that public health response activities are costlier for each actual case than the average costs of health care. Even though some children who contract measles will be hospitalized with a resulting substantial medical bill, 80% of cases will not need this level of care. The public health response will be similar for all proven cases.
Conclusion
Outbreaks of preventable illnesses have high potential economic costs. In this brief we explored the potential costs to the state for measles outbreaks with respect to costs of state-funded medical care and public health responses. Communities will never achieve a 100% measles immunization rate, as MMR dosing starts at one year of age. As long as individuals travel outside their community where they could potentially be exposed to measles, there will be the potential for an outbreak. What this exploration of costs demonstrates is that as immunization rates decline, the costs of an outbreak increase.
Our model highlights the broader implications of the economic burden of relaxing vaccine requirements by looking at medical costs and public health response costs as two forms of direct expenditures that could impact the Texas State budget during an outbreak. The emerging trend from this model suggests that as vaccination rates decrease, disproportionately more expenditure is required by the state for response and containment.
Future studies should incorporate other perspectives of cost. For example, this study did not include the medical costs incurred by the 48.6% of children who have medical insurance through commercial insurers. If these were included, the medical costs within a community would be significantly greater, as reimbursement from commercial insurers is normally higher than state-funded programs. Furthermore, those commercial payments must be attributed to the commercial payers and calculated separately from the state’s payments. We also chose to combine children with and without state-funded health care programs. In reality, the cost sharing between the state, local communities and commercial insurers for medical care is far more complicated. Additionally, we excluded the cost burden on families for measles-related illness or quarantine. In the case of a measles infection, these costs might include financial losses due to time out of school or work while in isolation or attending to a sick child. We focused on the short-term costs, but death and long-term disability from measles are also possible, which could lead to lasting personal and societal consequences. Each of these cost perspectives requires a separate calculation and will have unique, long-term implications for the state’s economy.
As a final note of caution, the per-child costs presented in this early model may seem low and could create a false sense of security. They represent individual average child costs, but when applied to the state’s population of 7.5 million Texas children, the medical costs of an outbreak range from $15.5 to $63.3 million, and the costs of a public health response range from $115 to $410 million. In addition, the costs presented only represent a potential measles outbreak, not mumps or rubella, which are also included in the MMR vaccine. The costs associated with diseases controlled by other vaccines are also not included. Each disease comes with its own unique implications for medical, public health and income costs. However, this exploration of the effect of lower vaccination rates on costs demonstrates that there is a potential for significant increased state and personal spending on otherwise preventable illnesses.
Acknowledgments
The author would like to thank Baker Institute staff — especially Kirstin Matthews and Jacquie Klotz — for feedback on the model and manuscript. This article is part of the 2022 Vaccine Policy Symposium. Support for dissemination of this report and other vaccine policy research was generously provided by a “Bridging Bioethics Research & Policy” grant from The Greenwall Foundation. For more information and other related research, visit the Baker Institute Vaccine Project webpage at https://www.bakerinstitute.org/vaccine-project.
Endnotes
[1] Gillian D. Sanders et al., “Recommendations for conduct, methodological practices, and reporting of cost-effectiveness analyses: Second panel on cost-effectiveness in health and medicine,” JAMA 316, no. 10 (2016): 1093-103, https://doi.org/10.1001/jama.2016.12195.
[2] “Child and Adolescent Immunization Schedule,” Centers for Disease Control and Prevention, last updated February 17, 2022, https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html; Committee On Infectious Diseases, “Recommended Childhood and Adolescent Immunization Schedule: United States, 2022,” Pediatrics 149, no. 3 (Febrauary 17, 2022), https://doi.org/10.1542/peds.2021-056056.
[3] Alexandra Bhatti et al., “A Comprehensive Assessment Of Child Care Vaccination Laws Across The US,” Health Affairs 41, no. 4 (April 2022): 589-597, https://doi.org/10.1377/hlthaff.2021.01205.
[4] Bhatti et al., “A Comprehensive Assessment”; Jacqueline K. Olive, Peter J. Hotez, Ashish Damania, and Melissa S. Nolan, “The state of the antivaccine movement in the United States: A focused examination of nonmedical exemptions in states and counties,” PLOS Medicine 15, no. 6 (2018): e1002578, https://doi.org/10.1371/journal.pmed.1002616.
[5] TX DSHS (Texas Department of State Health Services), “Vaccination Coverage Levels in Texas Schools,” last updated May 26, 2022, https://dshs.texas.gov/immunize/coverage/schools/.
[6] Priscilla Magalhaes Loze et al., “Vaccines are different: A systematic review of budget impact analyses of vaccines,” Vaccine 35, no. 21(2017): 2781-2793, https://doi.org/10.1016/j.vaccine.2017.03.088; Audrey C. Bangs et al., “The Clinical and Economic Impact of Measles-Mumps-Rubella Vaccinations to Prevent Measles Importations From US Pediatric Travelers Returning From Abroad,” Journal of the Pediatric Infectious Diseases Society 11, no. 6 (2022): 257-266, https://doi.org/10.1093/jpids/piac011.
[7] Paul A. Gastañaduy and James L. Goodson, “Measles (Rubeola),” Centers for Disease Control and Prevention, June 24, 2019, https://wwwnc.cdc.gov/travel/yellowbook/2020/travel-related-infectious-diseases/measles-rubeola.
[8] CDC (Centers for Disease Control and Prevention), “Measles (Rubeola),” September 16, 2022, https://www.cdc.gov/measles/cases-outbreaks.html.
[9] Andrew J. Wakefield, “MMR vaccination and autism,” Lancet 354, no. 9182 (1999): 949-50, https://doi.org/10.1016/S0140-6736(05)75696-8.
[10] Manisha Patel et al., “Increase in Measles Cases — United States, January 1–April 26, 2019,” Morbidity and Mortality Weekly Report 68, no. 17 (May 3, 2019), https://www.cdc.gov/mmwr/volumes/68/wr/mm6817e1.htm; Meredith G. Dixon et al., “Progress towards regional measles elimination - Worldwide, 2000-2020,” Morbidity and Motality Weekly Report 70, no. 45 (November 12, 2021), https://www.cdc.gov/mmwr/volumes/70/wr/mm7045a1.htm.
[11] Jamison Pike et al., “Societal Costs of a Measles Outbreak,” Pediatrics 147, no. 4 (April 1, 2021), https://doi.org/10.1542/peds.2020-027037.
[12] TX DSHS, “Vaccination Coverage.”
[13] “QuickFacts: Texas,” United States Census Bureau, 2021, https://www.census.gov/quickfacts/TX.
[14] Bangs et al., “The Clinical and Economic Impact of Measles-Mumps-Rubella Vaccinations”; Patel et al., “Increase in Measles Cases.”
[15] “Health Insurance Coverage of Children 0-18,” Kasier Family Foundation, 2019, https://www.kff.org/other/state-indicator/children-0-18/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D.
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s), and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.


