
To access the Spanish version of this policy brief, download the PDF on the left-hand sidebar.
The spread of the Zika virus is a brand new threat to the United States, Mexico, and the rest of the Americas. The virus itself, however, is not new. It was originally identified in Africa in 1947 and was associated with a narrow geographic area from Africa to Asia (Fauci and Morens 2016). Seemingly sequestered from the developed world, little resources were directed at understanding Zika, even after outbreaks occurred outside of the virus’ normal geographic range in 2007 and 2013 (World Health Organization 2016a).
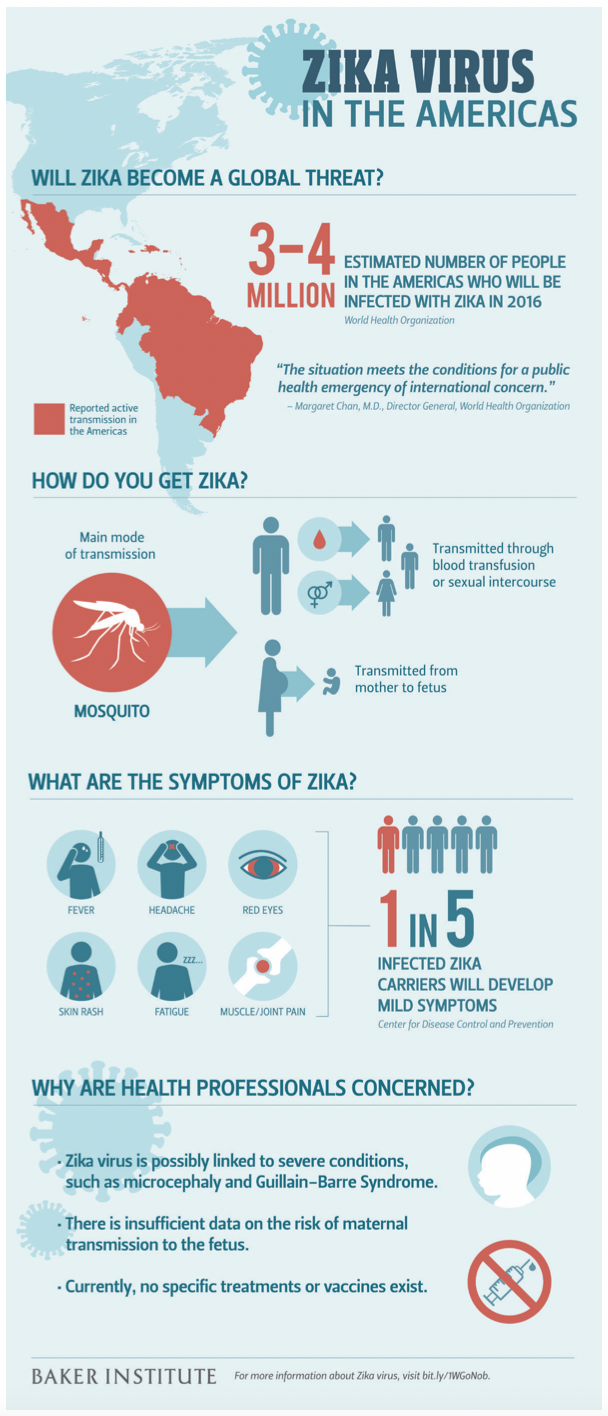
The outbreak of Zika in the Americas started in Brazil in early 2015, spreading quickly through the area and impacting an estimated 500,000 to 1.5 million individuals (WHO 2016b). Since that time, the virus also has quickly spread to 26 countries throughout the Americas, including Mexico and the United States (Pan American Health Organization 2016). In November 2015, Mexico reported three locally acquired cases of Zika (WHO 2015). The United States and its territories have experienced 52 cases of travel-related Zika virus infection. Puerto Rico and the U.S. Virgin Islands have reported nine total cases of locally acquired infection (Centers for Disease Control and Prevention 2016b). In addition, a case in Dallas, Texas, was confirmed to be sexually transmitted.
Similar to dengue (DENV), chikungunya (CHIKV), and West Nile virus (WNV), Zika is also an arbovirus that is spread primarily by mosquitos (Matthews and Herricks 2015). Specifically, Zika is a flavivirus—the same family of viruses as DENV and WNV. In the majority of cases, similar to DENV and CHIKV, Zika seems to cause an asymptomatic infection, so many may not even realize they have been infected (Matthews and Herricks 2015). Asymptomatic individuals can serve as virus reservoirs that can disseminate the virus if mosquitos take blood meals from those individuals, allowing those mosquitos to spread the virus to others who may develop a more severe infection. The most common symptoms of Zika are fever, rash, conjunctivitis (infection of the eye), and muscle and joint pain (CDC 2016b). The window from infection to symptom development has been estimated to be between three days and two weeks, but more data is needed to firmly determine the disease’s progression.
In addition to the mild symptoms, health authorities are concerned about the rising number of cases of Guillain-Barré syndrome (GBS) and microcephaly, which might be associated with the virus. GBS occurs when a person’s own immune system damages nerve cells in the body, typically caused by an over-reaction to an infection (CDC 2016b). As a result, the patient experiences muscle weakness and paralysis that can last from a few weeks to a few months; some will have permanent damage, and about one in 20 will die (CDC 2016b).
Microcephaly is a birth defect in which a baby’s head size is smaller than normal due to the brain’s arrested development during pregnancy. It can lead to seizures, developmental delays, intellectual disabilities, movement and balance issues, difficulty swallowing, hearing loss, and vision problems in a newborn (CDC 2016a). A recent study found that infants with microcephaly associated with congenital Zika infection have an increased risk for severe vision damage (de Paula Freitas, de Oliveira Dias, and Prazeres 2016).
There is not a definitive scientific link between Zika and GBS or microcephaly, but health authorities in Brazil noted a rise in both conditions soon after Zika became endemic in the region. As of January 2016, the Brazilian Ministry of Health has reported 4,783 cases of microcephaly and/or central nervous system defects, including 76 deaths, which is far higher than the average yearly rate of 163 cases of microcephaly in Brazil (WHO 2016b). Of those reported cases, 1,113 have been investigated, with Zika infection confirmed in 17 cases, two of which resulted in miscarriages (WHO 2016b). In the 76 reported deaths, Zika virus was identified in five of the cases (WHO 2016b). In 2015, Brazil reported a 19 percent increase in GBS; of 42 GBS cases identified in July 2015, 26 patients reported a history consistent with Zika infection (WHO 2016). Other countries with active Zika transmission have seen increases in GBS and are monitoring for microcephaly and other associated syndromes. From 2014 to 2015, French Polynesia reported a 10- to 20-fold increase in the incidence of microcephaly, which occurred after a 2013 Zika outbreak (WHO 2016b).
Both microcephaly and GBS have other known causes; therefore, further investigations are ongoing to confirm Zika as another cause (CDC 2016a, 2016b). But a major criticism of data linking Zika with GBS and microcephaly is that health authorities may be recognizing and reporting more cases of microcephaly and GBS due to recent heightened awareness. It is possible that Zika does cause these outcomes, but that only a subset of individuals will develop these more severe conditions.
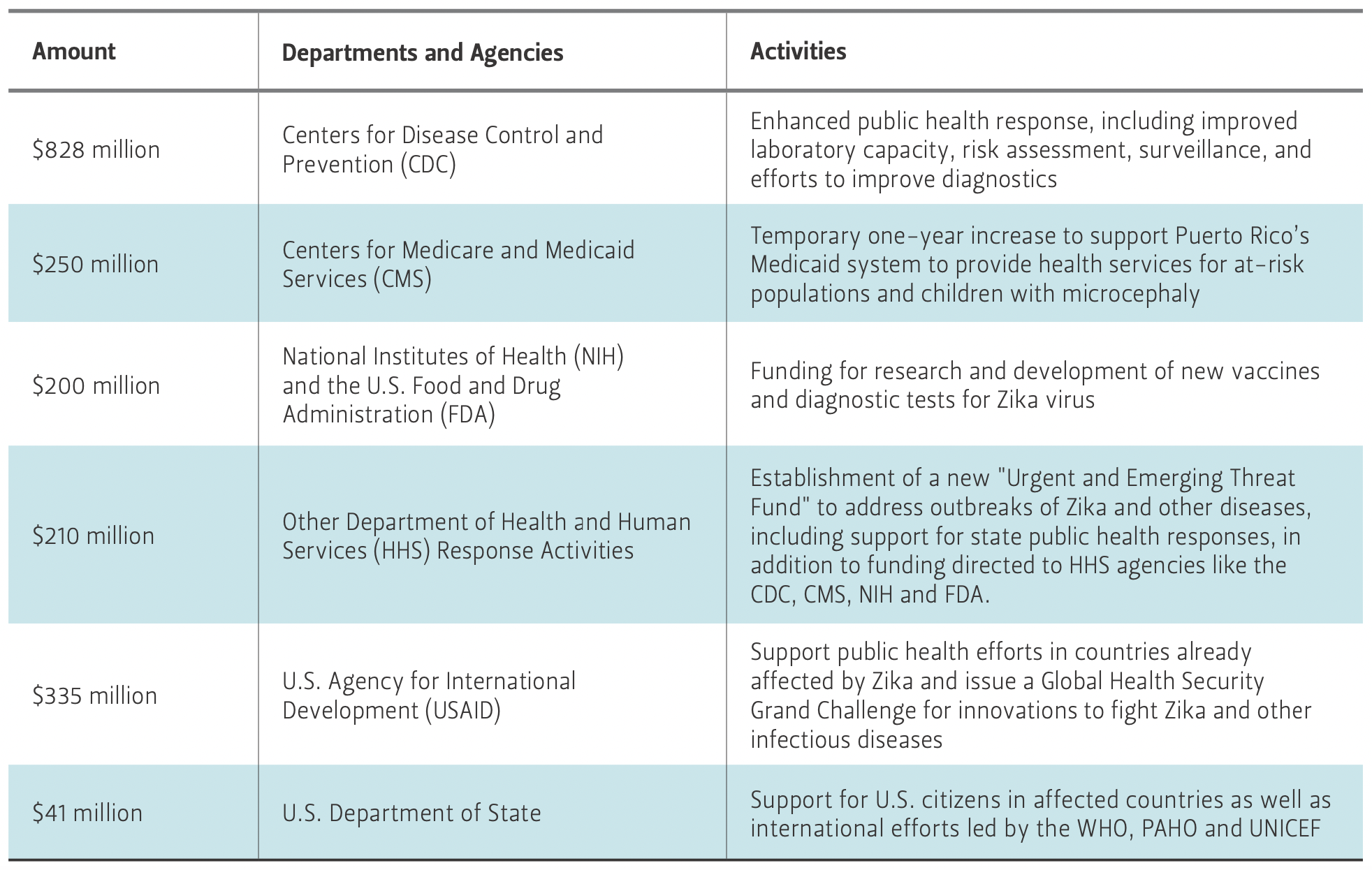
Table 1 — Breakdown of Proposed Emergency Zika Funding in the U.S.
Risk and Prevention
The priority now in the midst of a Zika epidemic is to obtain a better understanding of the Zika virus, including the virus infection rate, transmission, and health impact. Zika was identified in 1947 and yet little is known about the disease’s progression. The largest risk factor for the disease is exposure to mosquitos (Matthews and Herricks 2015). Sexual transmission is also possible. However, it is not known whether the Zika virus is also maintained in other bodily fluids, and it is unclear how long it remains in semen. Scientists believe the virus leaves the blood after a few weeks, but there has been concern for the potential of blood supply contamination, especially through donations from asymptomatic individuals (Franchini and Velati 2015).
In reaction to the Zika outbreaks—and more importantly, the fear that it could be linked to microcephaly and GBS—the White House announced that it would ask Congress for $1.8 billion in emergency funding to fight Zika, including conducting basic research on the virus, developing new treatments and vaccines, and studying the effect of Zika on fetal development (White House 2016). The proposed distribution of those funds, most of which are focused on national concerns, is outlined in Table 1.
On Feb. 11, 2016, the Brazilian government announced a collaborative grant between The University of Texas Medical Branch in Galveston, Texas, and the Evandro Chagas Institute in the Amazonian city of Belém in Brazil to develop a Zika vaccine (Goodman 2016). Meanwhile, the Brazilian Ministry of Health is working with the U.S. Centers for Disease Control and Prevention (CDC) on a vaccine partnership (Goodman 2016).
Recommendations
Vector Control
Typical mosquito control includes spraying for mosquitos outside at dusk and dawn. However, this strategy is not likely to work well for preventing Zika (as well as chikungunya and dengue). The particular type of mosquito that transmits Zika, the Aedes mosquito, has different behaviors than the more well-known Culex mosquitos that tend to live outdoors and are mostly active at dusk and dawn. In contrast, the “domesticate” Aedes mosquitos live around humans, including indoor environments, and are active during the day (Powell and Tabachnick 2013). To combat this, the Brazilian government recently authorized forced entry into private property to control the Aedes mosquito population.
Alternative vector control methods are currently being researched. Scientists have been working with microorganisms to reduce mosquito viral infections or longevity and are also trying to alter mosquito genetics to effectively sterilize males (which do not feed on blood) so that they cannot reproduce (Baldacchino et al. 2015). Most research indicates that there would be little, if any, negative impact of eradicating mosquitos, especially the species that carry diseases (Fang 2010).
Mosquito control is most effectively implemented by local health departments, which know their service areas well and can identify neighborhoods most in need. However, the United States has been criticized for not having enough well-resourced vector control programs to adequately protect its citizens (Herring 2010). Local, state, and national governments in the United States and Mexico should meet with local health departments and determine whether additional resources are needed for mosquito control.
Until we are able to eradicate mosquitos or more effectively prevent them from carrying and spreading disease, we must look to those who are most vulnerable in our population. In general, this will be people living in poverty, including the homeless, and those who do not have air conditioning and proper safeguards to prevent mosquitos from entering their homes, such as window screens. In addition, conditions of poverty in the United States and Mexico often are associated with environmental degradation and excess waste that create prime habitats for mosquito breeding. This likely will require local efforts to clean up areas near homes that may serve as mosquito breeding grounds. One such effort was recently announced in the city of Houston, Texas (City of Houston 2016).
Protections for Women of Childbearing Age
Until the threat of Zika to pregnant women and their fetuses is better understood, recommendations have been made for women who are pregnant or trying to become pregnant to avoid travel to areas that are experiencing Zika outbreaks. Several countries, including El Salvador and Colombia, have also recommended that women avoid getting pregnant in the near future in order to circumvent the risk of transmission—although this might not be realistic. Unfortunately, women who tend to have the least access to contraceptive methods are those of lower socioeconomic status. These women also are at a greater risk of acquiring Zika due to increased exposure to mosquitos and are least equipped to deal with the potential consequences of microcephaly.
Because these families may not have the ability to care for a child with microcephaly, pregnant women whose babies have tested positive for the condition may consider abortion. Abortion is legal in the United States and Mexico, but specific policies regarding when and under what circumstances abortions can be performed vary by state and in some cases are very restrictive (United Nations 2014). Complicating the issue is that microcephaly may not be detected until after 20 weeks of pregnancy, the threshold at which when abortion is illegal in many countries.
Fill the Gap on Other Critical Needs
In addition to mosquito control, there are several other areas of critical need to combat Zika. Surveillance of Zika, like other neglected tropical diseases (NTDs), is severely limited and needs to be improved. Furthermore, resources need to be directed toward basic research on the virus, development of a vaccine and treatment options, and support for individuals who have already been affected by Zika. The commitment of funds and other resources by the United States and other governments should help address the research and development gaps. However, there is little information or support for individuals or families that have been negatively impacted by Zika and are experiencing microcephaly
or GBS. In addition to the important goal of preventing further disease, some of the newly dedicated funds should be used to support individuals who have already been affected.
Conclusion
The 2014 Ebola and 2015–2016 Zika outbreaks are reminders of a very important lesson the developed world has taken for granted for far too long: Global health and NTDs can affect local health. If we continue to ignore infectious diseases that we see as rare and exotic, we will continue to see them arrive at our doorstep and cause panic. This can be prevented by continued investments in global health, especially in learning about emerging pathogens and determining ways to help those who are affected. In doing so, local public health will also be protected, as the tools to fight these diseases will have been developed long before they become a local problem in the developed world. This would also be the most cost-effective option, as preventing a crisis is always less expensive than reacting to one that has already occurred. Policymakers should keep this in mind when thinking about how to invest in global health.
References
Boldacchino, F., Beniamino Caputo, Fabrice Chandre, Andrea Drago, Alessandra della Torre, Fabrizio Montarsi and Annapaola Rizzoli. 2015. “Control methods against invasive Aedes mosquitos in Europe: a review.” Pest Management Science 71 (11):1471-1485.
Centers for Disease Control and Prevention (CDC). 2016a. “Birth defects: facts about microcephaly.” Accessed February 11. http://www.cdc.gov/ncbddd/birthdefects/microcephaly.html.
CDC. 2016b. “Zika Virus.” Accessed February 11. http://www.cdc.gov/zika/.
City of Houston. 2016. “City of Houston begins trash roundup to reduce mosquito breeding grounds.” Accessed February 12. http://www.houstongovnewsroom.org/go/doc/2155/2786322/.
de Paula Freitas, Bruno, João Rafael de Oliveira Dias, and Juliana Prazeres.
2016. “Ocular Findings in Infants With Microcephaly Associated With Presumed Zika Virus Congenital Infection in Salvador, Brazil.” JAMA Ophthalmology Epub ahead of print. doi: 10.1001/jamaophthalmol.2016.0267.
Fang, Janet. 2010. “Ecology: A world without mosquitos.” Nature 466: 432-434.
Fauci, Anthony S. and David M. Morens. 2016. “Zika Virus in the Americas – Yet Another Arbovirus Threat.” New England Journal of Medicine Epub ahead of print. doi:10.1056/NEJMp1600297.
Franchini, M. and Claudio Velati. 2015. “Blood safety and zoonotic emerging pathogens: now it’s the turn of Zika virus!” Blood Transfusion published online http://www.bloodtransfusion.it/articolosing.aspx?id=000763.
Goodman, J. 2016. “Brazil, Texas State Hospital Reach Deal on Zika Vaccine.” The New York Times, Accessed February 11.
Herring, M. E. 2010. “Where have all the vector control programs gone?” Journal of Environmental Health 73 (4): 30-31.
Kates, J., Josh Michaud and Allison Valentine. 2016. “Zika Virus: The Challenge for Women.” The Henry J. Kaiser Family Foundation. Accessed February 1. http://kff.org/global-health-policy/perspective/zika-virus-the-challenge-for-women/.
Matthews, K. R. and Jennifer R. Herricks. 2015. “Mosquito-Transmitted Epidemics: Dengue, Chikungunya and West Nile in the United States and Mexico.” Policy brief no. 12.16.15. Rice University’s Baker Institute for Public Policy, Houston, Texas.
Pan American Health Organization (PAHO). 2016. “Zika virus infection.” Accessed February 11. http://www.paho.org/zika.
Powell, J. R. and Walter J. Tabachnick. 2013. “History of domestication and spread of Aedes aegypti – A review.” Memórias do Instituto Oswaldo Cruz 108 Supplement 1: 11-17.
The White House. 2016. “Fact sheet: Preparing for and responding to the Zika virus at home and abroad.” Accessed February 8. https://www.whitehouse.gov/the-press-office/2016/02/08/fact-sheet-preparing-and-responding-zika-virus-home-and-abroad.
United Nations, Department of Economic and Social Affairs, Population Division. 2014. “Reproductive Health Policies 2014.” http://www.un.org/en/development/desa/population/publications/policy/reproductive-health-policies-2014.shtml.
UN, Department of Economic and Social Affairs, Population Division. 2015. “World Contraceptive Use 2015.” http://www.un.org/en/development/desa/population/publications/dataset/contraception/ wcu2015.shtml.
World Health Organization (WHO). 2015. “Zika virus infection – Mexico.” Accessed February 11, 2016. http://www.who.int/csr/don/03-december-2015-zika-mexico/en/.
WHO. 2016a. “TDR working with WHO on Zika response.” Accessed February 11. http://www.who.int/tdr/news/2016/collab-zika-response/en/.
WHO. 2016b. “Zika Situation Report: Neurological syndrome and congenital anomalies.” February 5. http://apps.who.int/iris/bitstream/10665/204348/1/zikasitrep_5Feb2016_eng.pdf?ua=1.
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s), and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.


