
Author(s)

Author's Note
The Baker Institute Drug Policy Program began in 2001. After an inaugural conference in April 2002, the first topic I chose to write about was needle exchange programs, a proven way to reduce the transmission of blood-borne diseases such as HIV/AIDS and hepatitis among injecting drug users. I chose needle exchange for a simple reason: I thought it made sense to advocate for a nonpartisan policy that would not only reduce suffering and save lives and money but, once its advantages were clearly delineated, would be embraced and enacted into law by Texas legislators. I was mistaken.
In this issue brief, I will summarize the scientific and fiscal evidence supporting needle exchange, trace recent developments, and recommend a framework for dealing with these and other aspects of drug use and abuse. The early and concluding sections are identical or quite similar to portions of my earlier writing on this topic.1
Terminology
In recent years, needle exchange programs (NEPs) began to be called Syringe Exchange Programs (SEPs), properly reflecting the fact that HIV and hepatitis viruses could live not only on the needle, but also within the syringe itself. Then, as established SEPs added distribution of condoms, offered information about avoiding disease, provided some primary health care and counseling, and connected people to treatment and recovery programs, they increasingly have come to be called Syringe Services Programs (SSPs), reflecting the wider scope of their offerings. Similarly, injecting drug users (IDUs) are increasingly referred to as PWID (People Who Inject Drugs), in recognition of the fact that injecting drug use is not the only relevant facet of their personhood. In this publication, I will use the newer labels.
Background
A contaminated needle is an extremely efficient transmitter of blood-borne disease, and the virus can live on a needle or within a syringe for as long as four days. Further, since the Centers for Disease Control and Prevention (CDC) estimates that at least a quarter of the people infected with HIV were unaware of it until they were diagnosed, and since the rapidity of infection with hepatitis C (HCV) results in an even greater percentage of unsuspecting carriers, needle users are key agents in the spread of these deadly epidemics.
The illegal drugs most commonly injected are heroin, cocaine, and methamphetamines, although each of these can be taken by other means, such as snorting, smoking, or ingesting orally. Prescription drugs can also be crushed into powder and made injectable. Using these drugs, particularly in the corrupted state in which they typically reach the retail market, is risky business. This inherent risk is substantially increased when users share needles contaminated by blood-borne diseases, most notably HIV/AIDS and hepatitis A, B, and C.
The actual result is stunning. Informed estimates of the number of PWID range from a quite conservative 1 million to a more common figure of approximately 1.2 million. By the end of 2002, according to the CDC, 32 percent of people living with AIDS in the United States were PWID, as were 28 percent of new diagnoses in that year.2
By 2015, the proportion of new HIV/ AIDS diagnoses had dropped to 9 percent and the CDC credited SSPs with playing a significant role in that decline.3 Hepatitis C, the most dangerous variant of that disease, is also rampant among PWID in the United States; surveys consistently find that 50 to 80 percent contract the virus within the first year of needle use and that it is found in the blood of 70 to 90 percent of all adult PWID. The lifetime cost of treating either of these diseases can easily exceed $300,000, much of which is paid by Medicaid, Medicare, local hospital districts, the U.S. Department of Veterans Affairs, and other public funds.4 Thus, every case of HIV/ AIDS or HCV prevented by syringe exchange carries an extraordinary cost benefit. In addition, SEPs take millions of potentially contaminated needles out of circulation instead of leaving them to be passed around or left in parks or public restrooms, where they could injure or infect children and others, including health workers and police who might receive needle-stick injuries in their contact with addicts.
The Science Is Clear
At least eight major studies, conducted by such organizations as the National Academy of Sciences, the CDC, the American Medical Association, and the World Health Organization, have unanimously concluded that access to clean needles dramatically reduces the incidence of blood-borne diseases and neither encourages people to start injecting drugs nor increases drug use by those who are already users. In addition, they serve as a bridge to treatment for a substantial minority of participants.
Syringe exchange is now an accepted part of public health programs in almost all countries of Western and Eastern Europe, Central Asia, and Australia and New Zealand. In some locales, sterile syringes can be exchanged at pharmacies, police stations, and even from specially designed vending machines. Even in Iran, the hyper-conservative ruling mullahs have approved of syringe exchange as a way to fight an HIV/ AIDS epidemic spread mainly by drug users.
Persuaded by scientific consensus and international examples, numerous U.S. cities have established SEPs that produce positive results. Most are in urban areas. Many are understaffed, underfunded, and unable to offer anything like the services that are needed. But when run well, they can dramatically reduce the spread of diseases. Two notable long-standing examples operate in Baltimore and New York City.
Baltimore
After the Baltimore City Needle Exchange, established in 1992, had been in operation for six years, the incidence of HIV in that city dropped by 35 percent overall and 70 percent among the approximately 10,000 participants in the program. By 2012, the percentage contracting HIV through injection had dropped from 53 percent to 12 percent.5 The Baltimore program, whose several vans provide clean needles at 16 locations, is such a standard part of the city's public health services that when snow halts its regular rounds, the news is carried on radio, TV, and Facebook right along with school closings.6
New York City
In New York City, the HIV rate among PWID climbed to 54 percent before the introduction of SSPs in the early 1990s. Thanks to SSPs and other prevention measures, it had fallen to 13 percent by 2001 and is now down to less than 1 percent. Epidemiologist Don Des Jarlais, director of research at New York’s Mount Sinai Beth Israel medical center and a leading expert on syringe exchange, said, “We appear to be very close to eliminating injecting-related transmission in a city with over 150,000 injecting drug users.”7
The Current Situation
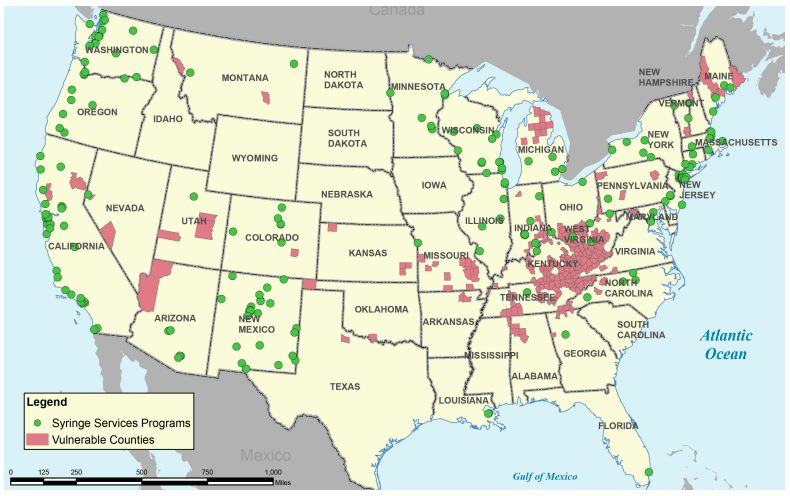
While the widespread attention currently given to opioid abuse stresses that addiction can happen anywhere, its incidence is hardly random. The map in Figure 1, prepared by the CDC in October 2016, shows (in pink) U.S. counties deemed to be particularly “vulnerable to rapid spread of HIV and hepatitis C infection among people who inject drugs.” Of 220 such counties in the nation, the most by far are concentrated in central Appalachia (Tennessee, Kentucky, West Virginia, southern Ohio, and Indiana). The green dots represent SSPs, none of which existed in this cluster of states in 2014. In addition to having four-fold increases in hepatitis C infections and comparable increases in HIV, these counties are also marked by “high unemployment and poverty, low educational attainment, and limited access to health care,” all factors known to contribute to drug abuse.8
Figure 1 — Counties Vulnerable to HIV/HCV & Locations of Syringe Services Programs (2016)
Typically, excess prescription of oral opioid painkillers such as oxymorphone (Opana), oxycodone (Oxycontin, a key ingredient in Percocet), hydrocodone (a primary ingredient in Lortab, Vicodin, et al.), and hydromorphone (Dilaudid) led to abuse and dependence, particularly among young (median age 32) white residents of rural communities and small towns. As their dependence increased and as reformulation of the drugs and restrictions on prescribing them made them harder to obtain, many users devised ways to crush pills into injectable form, which provided a quicker and more intense rush than ingesting them orally. Many turned to heroin, soon more readily available and cheaper, but also with no pharmaceutical label to indicate its strength. Eventually, in part because some dealers laced the heroin with fentanyl, an opioid estimated to be 20 to 50 times stronger than heroin, overdoses increased, too often resulting in death.
In the absence of SSPs or other ways to obtain sterile syringes legally, PWID shared those they could obtain, sharing disease in the process. As the opioid epidemic progressed, each state has been forced to confront its stubborn resistance to syringe exchange and to make some accommodation to settled science. Two cases in particular, Indiana and Kentucky, have particular relevance for ongoing public policy.
Indiana
After several years of an average five new diagnoses of HIV per year in the southeastern part of Indiana, 169 new cases appeared by mid-June 2015 and more than 20 new cases were being diagnosed every week. More than 80 percent of those also had HCV.10 The epicenter of the outbreak was Scott County, on the border with Kentucky, just north of Louisville. With no SSP, PWID had no legal way to obtain sterile syringes—possession of a needle without a prescription for medical use was a felony that carried a possible three-year prison sentence. They also had little opportunity to learn whether they were infected after spending cuts and thenGovernor Mike Pence’s opposition closed the Planned Parenthood office that had been the only HIV testing center in the county. As a result, drug users spread the virus by sharing needles. According to the Kentucky Standard, a huge majority of cases reported in Scott County were traced back to a single infected individual.11
Under pressure from public health officials in Indiana and elsewhere, and despite his opposition to SSPs, Governor Pence issued a temporary suspension of Indiana’s prohibition and allowed Scott County to set up a syringe exchange—for 30 days. Inevitably, as the epidemic did not wondrously disappear, that permission was extended to a year and then statewide, as other counties sought to avoid similar calamities.
Pence’s concession was not complete. Instead of embracing the public health model of preventing disease before it spreads, he backed legislation that required county officials to wait until increases in HIV and HCV were sufficient to justify declaring a public health emergency, then submit a plan to the state for approval to set up SSPs, with a time limit of one year. The state also provided little or no funding to help counties set up their programs. As a result, by the end of 2016, for every one of the fewer than 10 counties with programs underway, two others had failed to get started.12 Bureaucratic tensions and apparent turf wars among state, county, and nonprofit entities have contributed further to uneven progress.
The New England Journal of Medicine criticized Indiana’s reluctance to accept the reality that preventing the spread of blood-borne chronic diseases requires continuous access to sterile syringes.13 Similarly, a spokesman for the Foundation for AIDS Research said, “We must give Gov. Pence credit for finally doing the right thing in the end,” but he called the state’s HIV outbreak “entirely preventable…Indiana taxpayers could have been saved millions of dollars for treating those affected by the HIV outbreak if effective prevention policies were already in place.”14
In January 2017, Indiana Health Commissioner Jerome Adams pronounced SSPs to be a success, telling the Senate health committee that new cases of HIV had dropped from c. 22 per week at the 2015 peak to no more than three.15
Pence’s successor as governor, Republican Eric Holcomb, supported SSPs during his campaign, voiced strong support for existing programs after taking office (despite resistance from his attorney general), and pledged to give local communities more freedom to set up SSPs without having to go through the cumbersome process established in the previous administration. On February 1, 2017, the Indiana House voted 72-26 in favor of just such a measure. “Locals can act quickly when they become aware of an outbreak,” the author of the bill said. “If they have to wait the situation can get out of control quickly.”16
Kentucky
Pence’s example, however limited, may sway other governors and legislators who have been reluctant to accepts SSPs, but Kentucky’s experience will have a longer-lasting positive impact. As Scott County’s proximity to Louisville and its similarity to many rural counties in Eastern Kentucky suggest, the Bluegrass State also shared similar drug and disease problems. At least 1,248 people died of drug overdose in 2015, a 17 percent increase from 2014.17 In addition to a significant HIV problem, Kentucky had the highest rate of new HCV infections in the nation—4.1 per 100,000, nearly seven times higher than the national average of 0.6.18
In March 2015, just hours before the 2015 session ended, the Kentucky General Assembly passed an emergency measure that levied harsh penalties against heroin dealers, increased the availability of naloxone, and included a Good Samaritan provision that protected people from prosecution when seeking help for a person who has overdosed. It also permitted health departments to establish needle exchange programs if local jurisdictions approve.19 Predictably, departments and local newspapers embraced the opportunity, but because the bill provided no funding for SSPs, getting them off the ground was a challenge. Except for the first four years of the Obama administration, Congress had banned federal funding for syringe exchange since 1988. If the opioid crisis had broken out in Massachusetts or Oregon, the chances of overturning the ban would have been small. Fortunately, Kentucky had Republican friends in high places. Under pressure from constituent communities faced with the reality of increasing drug use and rising rates of disease, Representative Harold Rogers, chairman of the U.S. House Appropriations Committee, and Senate Majority Leader Mitch McConnell successfully tucked removal of the ban into the 2016 omnibus spending bill.20 Under the terms of the bill, federal funds can be used to pay staff, rent office space, provide vans, and cover other costs—but not to provide syringes or needles,21 a provision apparently included to allow reluctant legislators to assure their constituents, “I did not have needles with ‘those people.’”
Though warmly welcomed, the victory is not total. No additional funds were allocated for SSPs, so they must compete with other programs that depend on federal drug policy money, a slow process that will waste precious time in a situation where speed is crucial. An Oxford University study of a 1990s AIDS epidemic specifically identified SSPs as “the only measures that can target transmissions that happen within the first month.” Without such intervention,” one researcher observed, “the spread of HIV among drug-using populations is a public health time bomb.”22
Other states in the region—Ohio, Virginia, West Virginia, Tennessee, and North Carolina—have stepped aboard the SSP van, as have Massachusetts, Connecticut, and Vermont. New Jersey already had privately funded pilot SSPs, but in August 2016, Governor Chris Christie signed a bill that directed the health department to allocate $200,000 to programs that were running out of money to buy syringes.23 And, surprising to some, the conservative Utah Legislature, faced with high rates of overdose deaths and hepatitis C infections, not only legalized SSPs but allowed other public and private organizations “to take used needles from anyone and provide them with new, sterile ones in return.”24
The Texas Situation
In its latest count, the North American Syringe Exchange Network (NASEN) was aware of 228 SSPs in 35 U.S. states, Washington, D.C., Puerto Rico, and the Indian Nations.25 Others are known to exist under the radar. Taking its familiar place on so many measures of public welfare, Texas ranks dead last in making it legally possible for PWID to have access to sterile syringes, although a tiny number of sub rosa efforts exist and some pharmacies will sell syringes to PWID.
Needle exchange bills have been presented in every session of the Texas Legislature since the early 1990s, but were not taken seriously until 2005, when Senator Jon Lindsay, a respected Republican from Houston, authored a bill that would have made it legal for private individuals and organizations to fund and operate SEPs, not costing the state a cent but potentially saving millions of dollars. The bill did not come to a vote in the Senate.
In 2007, a similar bill sponsored by conservative Republican senator and physician Robert Deuell passed in the Senate by a 23-8 vote but was blocked in the House by the chair of the Public Health Committee, who refused to allow a committee vote. But in a little-heralded action in the same session, the Texas Legislature approved a comprehensive health measure that included a one-paragraph amendment that gave Bexar County permission to establish a pilot SEP.26
Bexar County’s district attorney at the time, however, recognized that the bill did not contain a clause exempting participants from possessing or distributing drug paraphernalia, which included syringes, and charged three program volunteers with a Class A misdemeanor, punishable by a $2,000 fine and up to a year in jail. The incident drew wide attention, most of it sympathetic to the volunteers and critical of the DA, but then-Attorney General Greg Abbott ruled that she had the legal right to exercise prosecutorial discretion and ignore the clear intent of the legislation. In the end, the volunteers did not go to jail, but the DA’s and Abbott’s decisions effectively shut down needle exchange in San Antonio for the last nine years, even though the enabling measure remains on the books and could be enacted in a favorable political climate and with cooperation from the current DA.
In 2009, the Senate passed Deuell’s bill again with equally bipartisan (23-6) support. The House version, sponsored by Representative Ruth Jones McClendon, D-San Antonio, went forward on a 7-3 vote from the Public Health Committee and, championed by mostly Republican medical personnel, was expected to win on the House floor. Instead, it was orphaned when the legislative clock ran down on the 140th day. Similar fate met similar bills in the 2011 and 2013 sessions, but Representative McClendon’s 2015 bill, which would have authorized pilot programs in seven counties—Bexar, Dallas, El Paso, Harris, Nueces, Travis, and Webb counties—or a hospital district in those counties, passed the House County Affairs Committee 9-0 and sailed through the House on a 92-37 vote. Since 2009, Senate supporters have opted to wait for the House to pass its version of the bill rather than mount another pointless run. Given the changed makeup of the Senate since the 2010 elections and Lt. Governor Dan Patrick’s longstanding opposition to SEPs, it is not clear McClendon’s new bill would have passed the Senate. In any case, for reasons not entirely clear, Patrick’s office did not assign the bill to an appropriate committee until it was too late to get a hearing.
Representative McClendon resigned from the Legislature in January 2016 because of illness. The effort to legalize SEPs during the 2017 legislative session is being led by Dallasarea Representative Toni Rose, author of HB 3256, quite similar to McClendon’s bill. Given the 2015 vote, the House will likely approve this bill. Given Patrick’s past votes against syringe exchange and the failure to get a Senate hearing in 2015, optimism is modest. Even if the bill passed both houses, it might still face a veto from now-Governor Abbott, who in 2015 vetoed a “Good Samaritan” bill that had passed the Senate by 30-1 and the House by 140-4. That veto would have been overridden had the governor not waited until after the legislative session ended to render his verdict.27
Harm Reduction
Like many organizations concerned with problematic drug use and ineffective drug policy, the Baker Institute Drug Policy Program advocates an approach known as harm reduction, which includes the following key principles, presented below almost verbatim from a longer list on the Harm Reduction Coalition website.28
- It accepts that licit and illicit drug use, for better or worse, is part of our world and cannot be eliminated by prohibition or punishment. A drug-free America is a fantasy and zero tolerance is a failed policy. It is possible and preferable, however, to minimize harmful effects rather than simply ignore or condemn them.
- It acknowledges that some ways of using even dangerous drugs are clearly safer than others and calls for appropriate nonjudgmental, non-coercive provision of services and resources to people who use drugs and to the communities in which they live.
- It affirms that drug users themselves can become important agents of reducing the harms of their use, sharing information, and supporting each other in strategies that meet the actual conditions of use.
Applied to syringe exchange, these principles have led to the development of an evolving set of “best practices,” including the following, excerpted from or based on a document prepared by the staff of the New York City Department of Health and Mental Hygiene and reflecting the consensus views of the nation’s leading syringe-exchange experts.29
- Maximize the number and variety of “access points” where PWID can obtain new and sterile syringes free of charge.
- Where possible, provide or coordinate provision of other services: food and clothing distribution, ancillary medical care (disease screening, vaccinations, some primary care), social services (e.g., housing, legal aid, drug abuse treatment), and counseling (e.g., safer sex, overdose prevention).
- Adapt the service delivery environment to the particular life circumstances of participants (e.g., non-English speakers, youth, homeless, undocumented workers, sex workers, LGBPTQ, et al.) and deliver services in a supportive, non-condemning and non-punitive matter.
- Provide as many syringes as PWID request at each transaction. Initially and still in many programs, programs have followed a one-to-one exchange requirement. Removing that requirement allows PWID to be sure they do not run out of sterile syringes in case they are unable to go to an SSP at the stated time. Existing evidence is strong that people who participate in SSPs are typically careful about returning their used syringes, both to avoid having the programs cancelled and also out of recognition that abandoned needles pose a danger to children and others.
- Promote and encourage “secondary syringe distribution” by permitting participants to distribute sterile syringes to people who for various reasons do not access the service directly. This can serve as a conduit for peer education when, for example, PWID who carry out secondary exchange provide safe injection information to those who are not accessing SSPs.
- Allow pharmacies to sell syringes without a prescription. Pharmaceutical associations favor syringe exchange, and the practice exists in some cities.
- Allow anonymous, confidential participation and minimize the data-collection burden on programs and participants. The desire of legislators and other officials to confirm that the programs are successful is understandable, and satisfying that desire may be necessary to initiate such programs, but the science is unambiguously clear. Syringe exchange works to reduce the spread of blood-borne diseases without increasing drug use. Burdening program participants and staff with compiling records beyond the basics—numbers of syringes distributed in a given period, numbers returned, and available data on HIV and hepatitis—is now a cumbersome, unnecessary burden on staff and a possible hindrance for participants.
Conclusion
No responsible person wants to encourage drug abuse. No fiscally prudent person wants to waste money simply to satisfy a sense of righteous indignation. No compassionate person wants to consign people unnecessarily to death or a living hell. Fortunately, providing people who inject drugs with access to sterile syringes allows us to be responsible, prudent, and compassionate—admirable criteria for good public policy.
Syringe exchange has been a bipartisan effort in the Texas Legislature. We urge all Republicans, Democrats, and Independents who believe in scientific evidence, public health, and compassion for others to contact their legislators, Lt. Governor Patrick, and Governor Abbott, and ask them to support bills establishing the legality of syringe exchange. It’s the right thing to do.
Endnotes
1. Earlier writings on this topic by William Martin are available at http://www.bakerinstitute.org/drug-public-health/.
2. “CDC HIV/AIDS Surveillance Report,” 2002, p.7, http://bit.ly/2lu6Xwv.
3. CDC, “HIV and Injection Drug Use, 2015, http://bit.ly/2kSBlxm.
4. New drugs for HCV, such as Harvoni and Sovaldi, are far more effective than older treatments, but they cost c. $90,000 for a 12-week treatment and may need to be repeated. At this point, Medicaid and most other insurers cannot afford to treat people with HCV.
5. “Needle Exchange Programs: Is Baltimore a Bust?” http://www.cipp.org/pdf/BALT_BUST.PDF.
6. Baltimore City Needle Exchange Program, http://health.baltimorecity.gov/node/439.
7. R. Knox, “Needle Exchanges Often Overlooked,” NPR, July 24, 2012, http://n.pr/2l3S6I8. Also, phone conversation with Don Des Jarlais.
8. B. Estep, “Needle exchanges spread,” Lexington Herald Leader, July 16, 2016, http://bit.ly/2kh8jpe.
9. Map, Reply, M.M. Van Handel, J.T. Brooks, Journal of Acquired Immune Deficiency Syndromes, March 2017, http://bit.ly/2lEiyFz.
10. S. Strathdee and C. Beyrer, “How to Stop the HIV Outbreak in Rural Indiana,” The New England Journal of Medicine (2015): 397- 399, http://bit.ly/2kTOhmO.
11. Kentucky Standard editorial, August 13, 2016, http://bit.ly/2kwQ7sR.
12. P. Demko, “Pence’s slow walk,” Politico, August 7, 2016, http://politi.co/2kxbtWP.
13. Strathdee and Beyrer, “How to Stop.”
14. See “Pence’s slow walk,” http://politi.co/2kxbtWP.
15. “Needle exchanges a success,” AP, January 12, 2017, http://bit.ly/2kwYogf.
16. “Needle-exchange bill OK’d by House,” Fort Wayne Journal Gazette, February 1, 2017, http://bit.ly/2keJwXQ.
17. See “Overdose deaths in 2015,” Insider Louisville, June 14, 2016, http://bit.ly/2lAIqBT.
18. See “First Reading of Budget,” SurfKY News, June 18, 2016, http://bit.ly/2lAHuNW.
19. Kentucky legislature passes emergency measures, March 27, 2015 entry, http://bit.ly/2lAHuNW.
20. See “Boost for needle exchanges,” Lexington Herald Leader, January 11, 2016, http://bit.ly/2l18f1o.
21. T. DeMio, “Will needle exchanges get boost?” Cincinnati Enquirer, February 22, 2016, http://cin.ci/2l1dQ83.
22. See Medical Press, November 8, 2016, http://bit.ly/2kxlCCX.
23. J. Ensslin, “Christie signs bill,” August 31, 2016, http://bit.ly/2kfco2j.
24. See “Utah legalizes needle exchange programs” AP, March 3, 2016, http://bit. ly/2l1d8HH.
25. See North American Syringe Exchange Network, https://nasen.org/.
26. See “Bexar County pilot SEP program,” http://bit.ly/2l1kJpH.
27. See Dallas Observer, June 3, 2015, http://bit.ly/2l1k33I.
28. Harm Reduction Coalition, “Principles of Harm Reduction,” http://bit.ly/2l1yaWN.
29. NYC Dept. of Health and Mental Hygiene, “Recommended Best Practices for SEPs,” http://bit.ly/2kiep8W.
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s), and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.

